Impeding rupture of a giant aortic root; surgical tips and tricks
| Available Online: | January, 2025 |
| Page: | 16–18 |
Author for correspondence:
Dr. Nikolaos G. Baikoussis, MD, MSc, PhD
Ippokrateio General Hospital of Athens
114 Vasilissis Sofias Avenue, 11537 Athens, Greece
E-mail: nikolaos.baikoussis@gmail.com
ISSN 2732-7175 / 2025 Hellenic Society of Vascular and Endovascular Surgery
Published by Rotonda Publications
All rights reserved. https://www.heljves.com
2Cardiology Department, Ippokrateio General Hospital of Athens, Greece
3Department of Cardiothoracic and Vascular Surgery, WestpfalzKlinikum, Kaiserslautern, Germany
Abstract
Full Text
References
Images
Abstract
Abstract:
We present an interesting and rare case of a 58-year-old man with a giant aortic root of 10 cm diameter along with the literature data; and tips and tricks in the surgical treatment.
Keywords: giant aortic root, huge aortic root, aortic aneurysm, aortic surgery, aortic rupture, impeding rupture of aortic root, aortic aneurysm.
Full Text
INTRODUCTION
Thoracic aortic aneurysm (TAA) in general is a silent disease which may have devastating complications. It is classified by the segment of the aorta involved. It is usually seen in men but all in all it is not a common disease – the incidence is estimated to be 6 to 10 cases per 100,000 patient-years. Etiology of the disease is multifactorial. Most aneurysms are degenerative and factors such as atherosclerosis and hypertension are highly associated, while many cases are caused by a wide range of disorders classified as aortitis. Syndromic TAA is a subcategory related to several connective tissue disorders such as Marfan, Ehlers-Danlos etc.
We herein report a case of giant aortic root measured 10 cm in its maximum diameter which was successfully treated with open surgical repair.
CASE
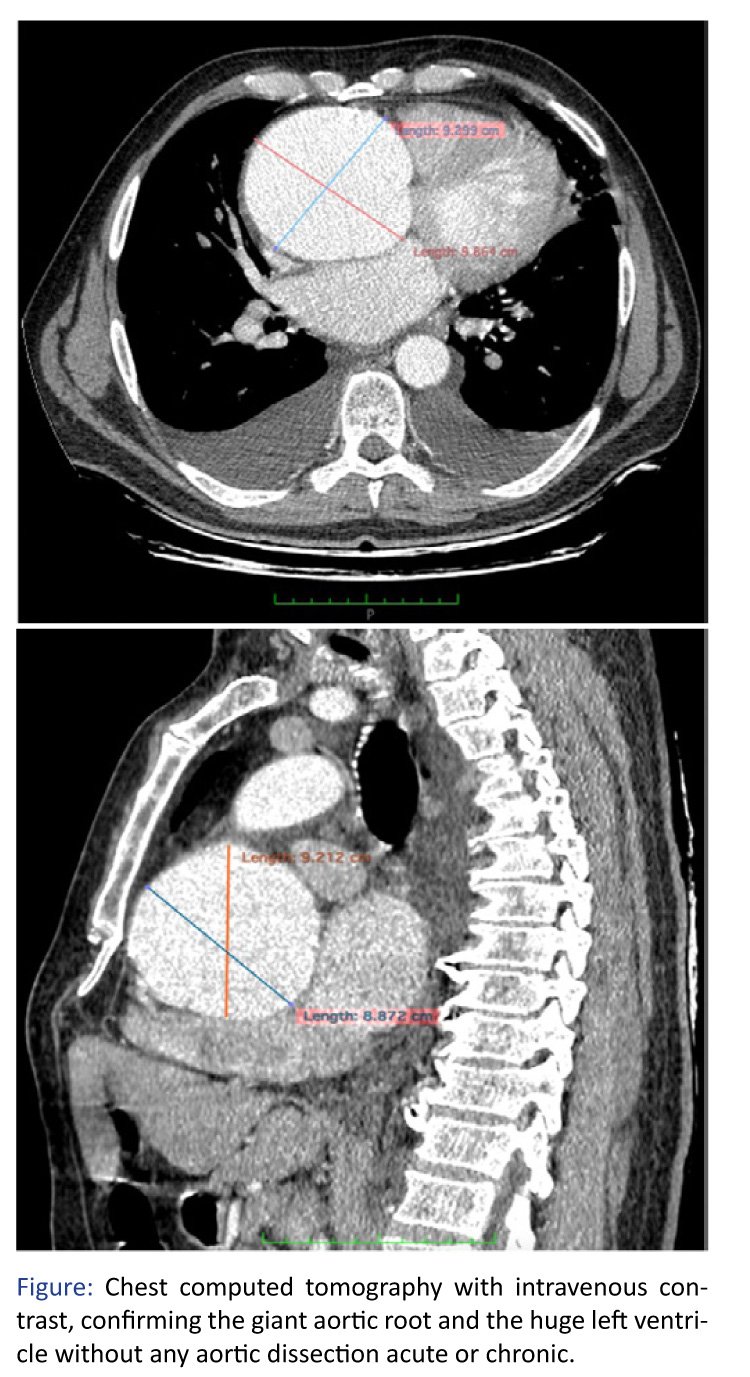
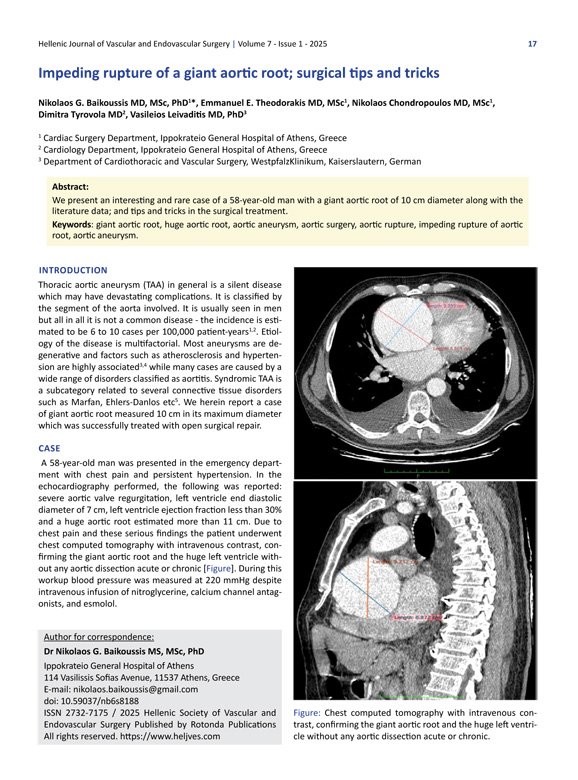
A 58-year-old man was presented in the emergency department with chest pain and persistent hypertension. In the echocardiography performed, the following was reported: severe aortic valve regurgitation, left ventricle end diastolic diameter of 7 cm, left ventricle ejection fraction less than 30% and a huge aortic root estimated more than 11 cm. Due to chest pain and these serious findings the patient underwent chest computed tomography with intravenous contrast, confirming the giant aortic root and the huge left ventricle without any aortic dissection acute or chronic [Figure]. During this workup blood pressure was measured at 220 mmHg despite intravenous infusion of nitroglycerine, calcium channel antagonists, and esmolol.
Chest pain was attributed to the pressure of the root to the surrounding tissues and in the impending rupture of the root. Due to these findings and the clinical presentation this case was considered as emergent and we decided to operate immediately.
After general anesthesia a typical right axillary artery cannulation was performed. A synthetic graft of 10 mm diameter was anastomosed to the subclavian artery in order to connect the arterial line of the extracorporeal circulation. Fully heparinization was done in order to be ready in case of any event like root rupture. Median sternotomy was performed and fibrosis and adhesions were recognized around the heart and aorta. Meticulous lysis of adhesions helped us to harvest the right atrium for the venous cannulation and then, we harvested the whole aortic root. Retrograde cardioplegia infusion was impossible due to adhesions. Antegrade through root vent was also impossible due to aortic root regurgitation. Thus, after clamping the ascending aorta; aortotomy was performed and cardioplegia was infused directly in the coronary ostium.
The aortic root was excised and the buttons of both coronary arteries were prepared appropriately with mobilization in order to approximate the graft of the upcoming Bentall procedure. After appropriate sizing a valved Valsalva graft with mechanical aortic valve of 27 mm and 30 mm ascending aorta graft (Carboseal Valsalva graft) was used. Then, a typical Bentall procedure was performed. The early postoperative course was uneventful and the patient was discharged in the fifth postoperative day. The patient at 3 months reports enhanced performance status and follow-up imaging demonstrated improved LV function and properly working aortic valve. Nine-month follow up revealed no surprises as the patient is fully active and new laboratory and ultrasound workup demonstrated no abnormalities.
DISCUSSION
Open surgical repair is considered to be the gold standard for managing thoracic ascending aortic aneurysms and dissection. Aortic root involvement necessitates coronary artery re-implantation and maybe aortic valve replacement or repair. In case both ascending aorta and valve are diseased, valve replacement is necessary and modified Bentall procedure is most commonly used.
In case of a giant root, some tips and tricks are useful for patient safety. Axillary artery cannulation is performed before sternotomy in order to be safe in case of root rupture. If needed, in some cases, venous cannulation through femoral vein may be also performed before sternotomy and start cooling of the patient. Fully heparinization of the patient is done early, before sternotomy, to be ready for extracorporeal circulation immediately. The two buttons of the coronary arteries are in a certain distance and their approximation anastomosis to the synthetic graft may require extended mobilization of both coronaries or elongation with the interposition of a synthetic graft of 8 mm in diameter.
Nowadays, aortic valve repair in case of regurgitation is considered to be a safe alternative. Valve-sparing aortic root replacement is recommended for patients without significant aortic valvular disease. So, in these cases, aortic valve repair may be performed and only substitute the root, the ascending aorta and anastomose the coronary buttons to the graft. This way the Bentall procedure and the mechanical valve may be avoided. In case of valve repair, if the aortic annulus is extremely dilated, repair may be difficult and the long-term results, doubtful. Techniques with ring implantation are applied. However, in our case factors such as severe aortic valve regurgitation and poor LV function led us to decide that valve replacement was the optimal choice for the patient. At the end of the procedure intraoperative transesophageal echocardiography is mandatory to evaluate the competence of the repaired valve.
References
1 Bickerstaff LK, Pairolero PC, Hollier LH, Melton LJ, Van Peenen HJ, Cherry KJ, Joyce JW, Lie JT. Thoracic aortic aneurysms: a population-based study. Surgery. 1982 Dec;92(6):1103-8. PMID: 7147188.
2 Clouse WD, Hallett JW Jr, Schaff HV, Gayari MM, Ilstrup DM, Melton LJ 3rd. Improved prognosis of thoracic aortic aneurysms: a population-based study. JAMA. 1998 Dec 9;280(22):1926-9. doi: 10.1001/jama.280.22.1926. PMID: 9851478.
3 Ferro CR, de Oliveira DC, Guerra Fde F, de Lucena AJ, Nunes FP, Ortiz ST, Egito ES, de Sousa LC, Jatene AD, Piegas LS. Prevalence and risk factors for combined coronary artery disease and aortic aneurysm. Arq Bras Cardiol. 2007 Jan;88(1):40-4. English, Portuguese. doi: 10.1590/s0066-782×2007000100007. PMID: 17364117.
4 Booher AM, Eagle KA. Diagnosis and management issues in thoracic aortic aneurysm. Am Heart J. 2011 Jul;162(1):38-46.e1. doi: 10.1016/j.ahj.2011.04.010. Epub 2011 Jun 15. PMID: 21742088.
5 Coady MA, Davies RR, Roberts M, Goldstein LJ, Rogalski MJ, Rizzo JA, Hammond GL, Kopf GS, Elefteriades JA. Familial patterns of thoracic aortic aneurysms. Arch Surg. 1999 Apr;134(4):361-7. doi: 10.1001/archsurg.134.4.361. PMID: 10199307.
6 Zehr KJ, Orszulak TA, Mullany CJ, Matloobi A, Daly RC, Dearani JA, Sundt TM 3rd, Puga FJ, Danielson GK, Schaff HV. Surgery for aneurysms of the aortic root: a 30-year experience. Circulation. 2004 Sep 14;110(11):1364-71. doi: 10.1161/01.CIR.0000141593.05085.87. Epub 2004 Aug 16. PMID: 15313937.
7 Bentall H, De Bono A. A technique for complete replacement of the ascending aorta. Thorax. 1968 Jul;23(4):338-9. doi: 10.1136/thx.23.4.338. PMID: 5664694; PMCID: PMC471799.
8 Youssefi P, Zacek P, Debauchez M, Lansac E. Valve-Sparing Aortic Root Replacement Using the Remodeling Technique With Aortic Annuloplasty: Tricuspid Valves With Repair of Specific Lesion Sets: How I Teach It. Ann Thorac Surg. 2019 Jun;107(6):1592-1599. doi:10.1016/j.athoracsur.2019.03.013. Epub 2019 Apr 3. PMID: 30953656.
Images