An urgent axillopopliteal bypass to treat a bleeding infected anastomotic groin pseudoaneurysm
| Available Online: | January, 2025 |
| Page: | 19–20 |
Author for correspondence:
Melina S. Stathopoulou
Department of Surgery, Patras University Hospital, Patras, Greece
E-mail: MelinaStath@gmail.com
ISSN 2732-7175 / 2025 Hellenic Society of Vascular and Endovascular Surgery
Published by Rotonda Publications
All rights reserved. https://www.heljves.com
2Department of Internal Medicine, Division of Infectious Diseases, Patras University Hospital, Greece
3Department of Radiology, Patras University Hospital, Greece
Full Text
References
Images
Full Text
INTRODUCTION
A 59-year-old male was transferred from a local hospital with a bleeding sinus at his left groin, controlled with external bandaging. He had previously undergone a femorofemoral bypass due to left leg claudication five years ago, an aortobifemoral bypass three years ago, and a graft extension of the left limb to the profunda one year ago for thrombotic complications. Postoperatively, a left groin infection was treated with debridement, leading to a draining sinus. Eventually, a massive bleeding occurred through this sinus six months later.
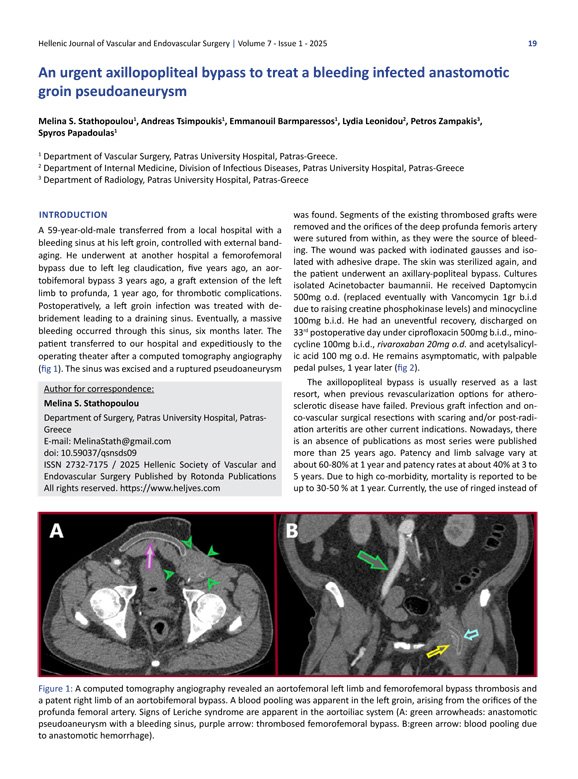
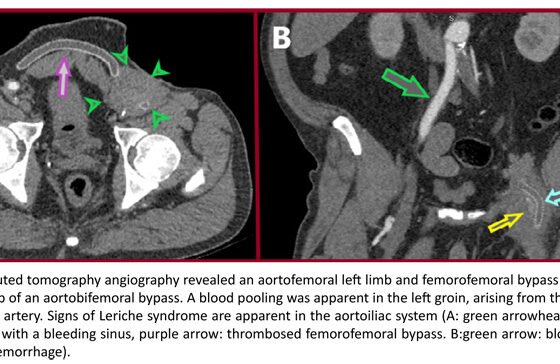
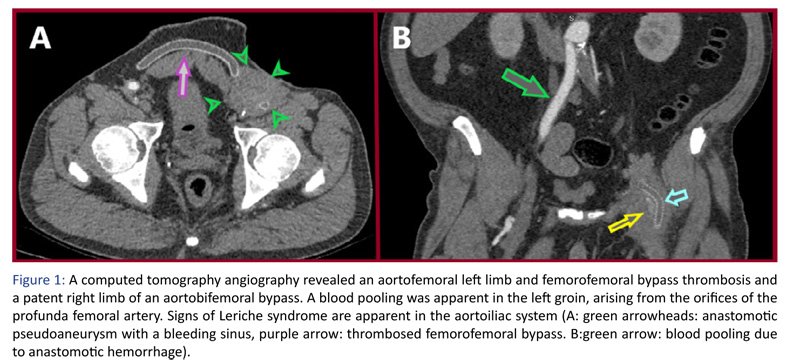
The patient was transferred to our hospital and taken expeditiously to the operating theater after a computed tomography angiography (Fig. 1). The sinus was excised, and a ruptured pseudoaneurysm was found. Segments of the existing thrombosed grafts were removed, and the orifices of the deep profunda femoris artery were sutured from within, as they were the source of bleeding. The wound was packed with iodinated gauzes and isolated with adhesive drape.
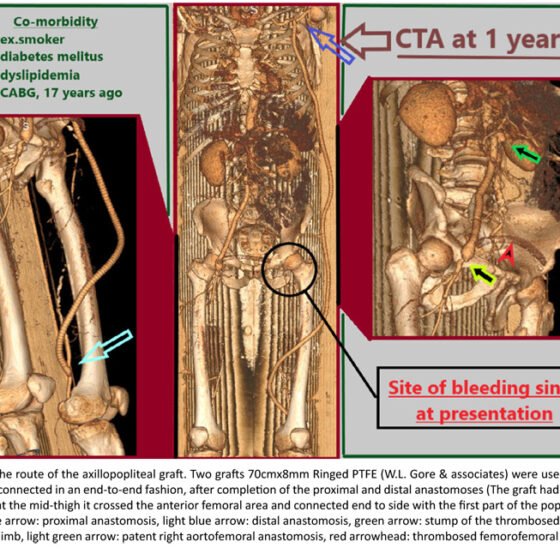
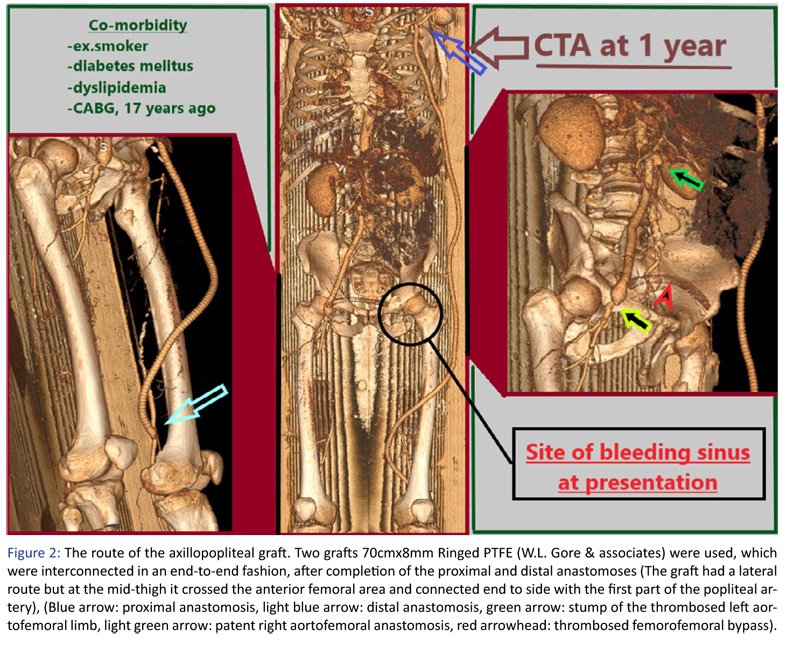
After sterilization of the skin, the patient underwent an axillary-popliteal bypass. Cultures isolated Acinetobacter baumannii. He received Daptomycin 500 mg o.d. (eventually replaced with Vancomycin 1 g b.i.d. due to rising creatine phosphokinase levels) and Minocycline 100 mg b.i.d. He had an uneventful recovery and was discharged on the 33rd postoperative day under Ciprofloxacin 500 mg b.i.d., Minocycline 100 mg b.i.d., Rivaroxaban 20 mg o.d., and Acetylsalicylic acid 100 mg o.d. He remains asymptomatic, with palpable pedal pulses, one year later (Fig. 2).
The axillopopliteal bypass is usually reserved as a last resort when previous revascularization options for atherosclerotic disease have failed. Previous graft infection and onco-vascular surgical resections with scarring and/or post-radiation arteritis are other current indications. Nowadays, there is an absence of publications, as most series were published more than 25 years ago. Patency and limb salvage vary at about 60–80% at one year, and patency rates are about 40% at 3 to 5 years. Due to high comorbidity, mortality is reported to be up to 30–50% at one year. Currently, the use of ringed instead of unsupported PTFE grafts, 8mm in diameter (vs 6mm in older trials), and the modern antithrombotic treatment (anticoagulation plus antiplatelets based on the Voyager-Pad trial) may give better results.
{kind=link}
{kind=link}