Open surgical repair of a giant iatrogenic pseudoaneurysm of the profunda femoris artery. A report of a case

| Available Online: | October, 2025 |
| Page: | 162–164 |
Author for correspondence:
Christos Argyriou, MD
Assistant Professor of Vascular Surgery, 8 Lordou Vyronos str., Alexandroupolis, Greece, 68131
Tel: +30 6944359751
E-mail: argchristos@hotmail.com, cargyriou@med.duth.gr
doi: 10.59037/bxp9sq07
ISSN 2732-7175 / 2025 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Christos Argyriou, Nikolaos Rousas, Stavros Parisidis, Nikolaos Triantafyllou, Konstantinos Dimitriadis, George S. Georgiadis
Department of Vascular Surgery, Medical School, “Democritus” University of Thrace, University General Hospital of Alexandroupolis, Thrace, Greece
Full Text
Gallery
Full Text
Abstract:
We report the case of a 92-year-old male patient who suffered from a 9cm in diameter iatrogenic pseudoaneurysm (PA) of the profunda femoris artery (PFA) and managed surgically by excision and interposition of an autologous bypass. Femoral artery PAs are the most common iatrogenic arterial injuries caused by femoral artery catheterizations. In particular, pseudoaneurysms of the PFAs can remain clinically silent but are potentially lethal if not diagnosed or treated promptly. Endovascular or minimally invasive techniques are usually the preferred first-line treatment options, however in challenging cases surgical reconstruction remains the most successful definitive treatment.
Keywords: deep femoral artery peudoaneurysm, iatrogenic arterial pseudoaneurysm, surgical repair.
INTRODUCTION
Femoral artery pseudo-aneurysm (PA) results from a variety of mechanisms including blood-borne infections, trauma, injection of illegal substances, arterial access for diagnostic and endovascular procedures, closure devices, synthetic graft infections and chronic anastomotic degeneration of bypass grafts. In particular, iatrogenic PA of the profunda femoris artery (PFA) is a classical complication of arterial percutaneous diagnostic angiography or interventional procedures which occurs in 0.2-2.6% of cases1. We describe the case of a 92-year-old male patient who suffered from a giant 9cm-diameter iatrogenic pseudo aneurysm of the PFA artery, managed surgically.
CASE REPORT
A 92-year-old male patient was admitted to the cardiology department for suspected endocarditis following a 14-day period of fever of unknown etiology. Trans-esophageal echocardiogram and positive blood cultures for gram-positive cocci (Staphylococcus Aureus) confirmed the diagnosis. The patient had a medical history of transcatheter aortic valve replacement one year ago and atrial fibrillation under anticoagulant treatment. From the 1st day of the admission the patient reported an increasing discomfort in his left mid-thigh which gradually turned into a worsening, non-remitting pain. At clinical examination, a significant femoral swelling and pulsating painful mass in the suspected region was palpated while his hemoglobin level had dropped from 10.5mg/dl on admission to 7.2md/dl.
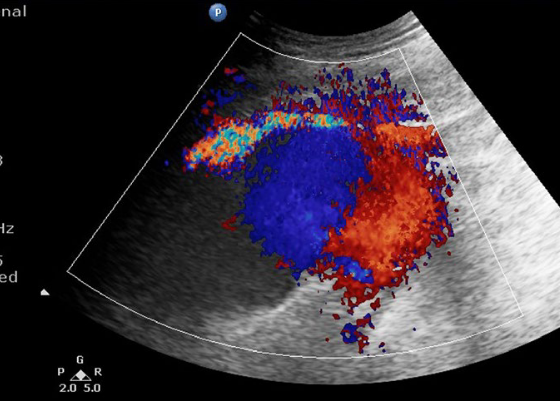
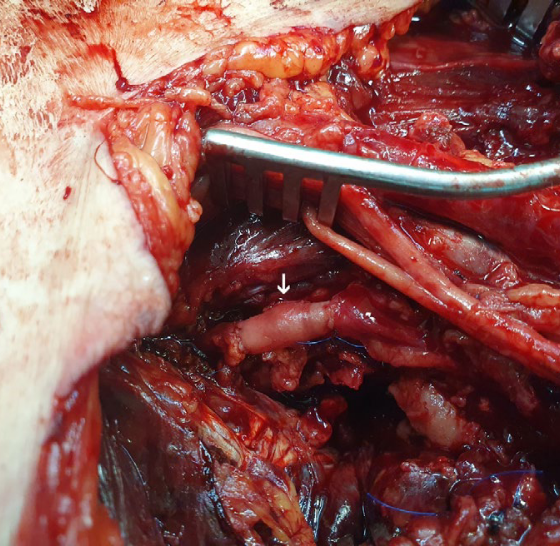
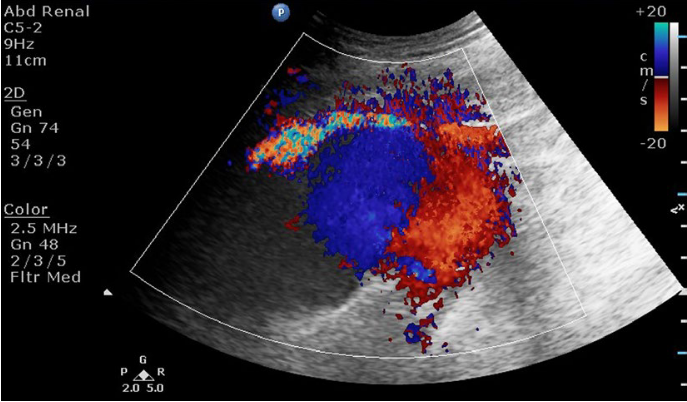
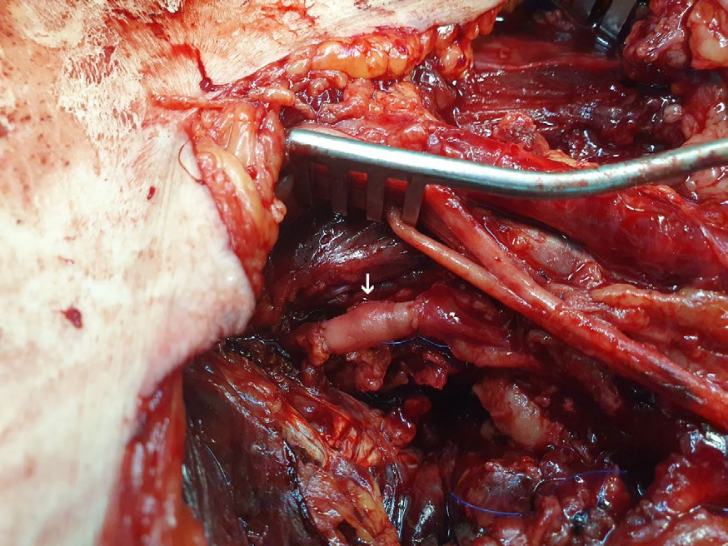
Ultrasound color-duplex scanning using a 5-MHZ convex array transducer revealed a giant (9-cm in diameter, 5-cm in length) expanding PFA pseudoaneurysm, located approximately 5-cm distal to the femoral bifurcation, between the 2nd and 3rd perforating artery (Figure 1). While an endovascular option was initially considered as an attractive solution due to its minimally invasive nature, the advanced patient’s age and his current anticoagulation treatment, we opted for open surgical repair. Therefore, through a long midline left groin incision, the first perforating branch of the deep femoral artery PA was dissected and excised while reconstruction was completed by interposition of an autologous bypass using segment of the distal ipsilateral greater saphenous vein (Figure 2). Perioperatively, 4 units of packed red blood cells were transfused. The patient had an uneventful recovery, having a mild wound lymphorrhea treated conservatively with elastic compression, completely resolving at 3 months post-operatively.
DISCUSSION
Pseudoaneurysms are reported to occur in 1% of diagnostic arteriograms and up to 8% of therapeutic endovascular interventions2. The most frequent complications range from 0.5% to 8% and include hematoma, uncontrollable groin and/or retroperitoneal bleeding, PA formation, arteriovenous fistula, and in situ arterial dissection with or without associated thrombosis2. Less frequent complications include distal embolization, nerve damage, abscess, and lymphocele2. In recent years, a number of percutaneous closure devices have been developed, with the hope of reducing the frequency of local complications and allowing early patient mobilization post endovascular intervention. However, these studies failed to demonstrate a reduction in local complications associated with the use of these devices3.
Endovascular repair of femoral arterial access complicaOpen surgical repair of a giant iatrogenic pseudoaneurysm of the profunda femoris artery. A report of a casetions is considered an attractive solution in patients who cannot tolerate vascular reconstruction and bleeding due to advanced cardiovascular disease. Coil embolization is the mainstay of endovascular treatment for PFA injury and has been reported to achieve a technical success rate exceeding 90%4. However, it may be unsuitable for large pseudoaneurysms (>4 cm), wide-neck lesions (>1 cm), or cases requiring preservation of DFA perfusion4. In contrast, stent grafting can be applied even in such challenging cases, enabling rapid hemostasis by sealing the bleeding point within the pseudoaneurysm due to nitinol stent technology allowing increased resistance to external compression and bending stress5.
Ultrasound-guided compression is an effective treatment for pseudoaneurysm of the PFAs, with success rates ranging from 70% to 90% in patients without anticoagulation therapy6. Nevertheless, this method has significant limitations. It is painful and time-consuming, with suboptimal results in patients who are obese and under anticoagulant treatment7. As an alternative, direct percutaneous embolization of the PA sac with different embolic materials has been reported. Thrombin is the most popular embolic agent used for percutaneous occlusion of femoral PAs because it causes fast and efficient thrombosis in the aneurysmal sac without filling it with foreign material. However, some complications may occur with this agent, including allergic reaction and distal thrombosis of the parent artery by leakage through the PA neck8. Comparing these two methods, the only randomized clinical trial existing in the literature concluded that percutaneous thrombin injection appeared to be more effective than ultrasound-guided compression in achieving primary thrombosis of a pseudoaneurysm, although other case series in the literature have reported higher thrombosis rates with compression compared to previous case series7,9.
N-butyl-2 cyanocrylate (NBCA) glue is a potential alternative to thrombin, initially described or treating arterio-venous malformations amenable to endovascular interventions10. However, its main drawback is the risk of direct percutaneous embolization with NBCA glue is distal embolization due to escape of the material from the pseudoaneurysmal sac before it is completely polymerized10. In the era of endovascular evolution, surgical treatment of femoral PAs is less common but can be life-saving, especially when other modes of intervention are more likely to fail or are contraindicated. In our patient, obesity, a small-neck with a large diameter deep femoral PA surrounded by an extended hematoma were unsuitable factors for endovascular or minimally invasive strategy. Further selection criteria for open surgical reconstruction were the rapidly expanding pseudoaneurysm from the continuous intrasac bleeding and worsening neuropathy due to local compression symptoms of the femoral nerve. In this regard, resolution of the symptoms would be improved only after surgical decompression of the hematoma and vascular reconstruction.
CONCLUSION
Femoral PAs are relatively common iatrogenic injuries following therapeutic and diagnostic catheterization procedures. Although endovascular or minimally invasive techniques have been evolving and transforming into the gold-standard treatment option, surgical reconstruction PFA pseudoaneurysms still remain the sine qua non of vascular repair, especially in selected cases not amenable to endovascular solutions.
REFERENCES
- Katzenschlager R, Ugurluoglu A, Ahmadi A, Hülsmann M, Koppensteiner R, Larch E, Maca T, Minar E, Stümpflen A, Ehringer H. Incidence of pseudoaneurysm after diagnostic and therapeutic Radiology. 1995 May;195(2):463-6.
- Etemad-Rezai R, Peck DJ. Ultrasound-guided thrombin injection of femoral artery pseudoaneurysms. Can Assoc Radiol J. 2003 Apr;54(2):118-20.
- Koreny M, Riedmüller E, Nikfardjam M, Siostrzonek P, Müllner M. Arterial puncture closing devices compared with standard manual compression after cardiac catheterization: systematic review and meta-analysis. JAMA. 2004 Jan 21;291(3):350-7.
- Watanabe S, Kanazawa R, Uchida T, Higashida T, Yamazaki K, Kono T: Endovascular embolization of femoral pseudoaneurysm associated with therapeutic and diagnostic neuroendovascular procedures. J Neuroendovasc Ther. 2023, 17:8-14.
- Morgan R, Belli Current treatment methods for postcatheterization pseudoaneurysms. J Vasc Interv Radiol. 2003 Jun;14(6):697-710.
- Lange P, Houe T, Helgstrand UJ. The efficacy of ultrasound-guided compression of iatrogenic femoral pseudo-aneurysms. Eur J Vasc Endovasc Surg. 2001 Mar;21(3):248-50.
- Cox GS, Young JR, Gray BR, Grubb MW, Hertzer Ultrasound-guided compression repair of postcatheterization pseudoaneurysms: results of treatment in one hundred cases. J Vasc Surg. 1994 Apr;19(4):683-6.
- Ergun O, Çeltikçi P, Güneş Tatar İ, Yılmaz M, Hekimoğlu Percutaneous thrombin injection treatment of a femoral artery pseudoaneurysm with simultaneous arterial balloon occlusion: Case report and review of the literature. Turk Kardiyol Dern Ars. 2016 Dec;44(8):684-689.
- Lönn L, Olmarker A, Geterud K, Klingenstierna H, Delle M, Grip L, Risberg B. Treatment of femoral pseudoaneu Percutaneous US-guided thrombin injection versus US-guided compression. Acta Radiol. 2002 Jul;43(4):396400.
- Parihar A, Tomar S, Phadke RV. Direct sac puncture and glue embolization of intraosseous AVM of the Int J Oral Maxillofac Surg. 2011 Jul;40(7):749-52.
{kind=link}
{kind=link}