Open repair of a distal mesenteric artery mycotic aneurysm: Keep as many collaterals as possible

| Available Online: | October, 2025 |
| Page: | 158–161 |
Author for correspondence:
George S. Georgiadis
Professor of Vascular and Endovascular Surgery “Democritus” University of Thrace, University General Hospital of Alexandroupolis, Dragana Area, Alexandroupolis, Greece, 68100
Tel: +30 6944299711
E-mail: ggeorgia@med.duth.gr, georgiadis.vasc@gmail.com
doi: 10.59037/3fnje697
ISSN 2732-7175 / 2025 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
George S. Georgiadis1, Konstantinos Dimitriadis1, Savas P. Deftereos2, Christos Argyriou1
1 Department of Vascular Surgery, Medical School, “Democritus” University of Thrace, University General Hospital of Evros, Alexandroupolis, Greece
2 Department Radiology, Medical School, “Democritus” University of Thrace, University General Hospital of Evros, Alexandroupolis, Greece
Abstract
Full Text
Gallery
Abstract
Mycotic superior mesenteric artery (SMA) aneurysms are very rare with a significant risk of rupture and high mortality rate. Current guidelines recommend an endovascular first line approach but open repair is still an option when anatomical constrains exist. We present a symptomatic, 28mm in diameter, partially thrombosed mycotic pseudoaneurysm of the distal SMA, originating from infective endocarditis. Emergent open surgical repair was performed. Our strategy included careful dissection of the aneurysm to preserve the intestinal vascular arcades, keeping as many collaterals as possible. After aneurysm resection, in-situ reconstruction using an interposition saphenous vein graft was performed. Patient course was uneventful. Two weeks later the patient underwent successful aortic valve replacement. A follow-up examination at 3 years founds the patient asymptomatic.
Full Text
INTRODUCTION
Visceral aneurysms though rare, have an insidious onset and can be potentially lethal or lead to catastrophic complications if not diagnosed or treated promptly1,2. Traditionally, surgery represented the treatment of choice offering the advantage of durability, reduced need for follow-up studies and low mortality rates whereas percutaneous/endovascular solutions have emerged as alternative attractive management solutions due to its minimal invasiveness, efficacy and low rates of complications in selected cases3,4. Moreover, endovascular embolization is only feasible if after treatment the end organ perfusion will be guarantee by the collateral flow and if the inflow and outflow vessels can be accessed and occluded by a catheter-based system5.
In the presence of an adequate collateral flow (splenic artery, celiac trunk, proximal superior mesenteric artery and common hepatic artery), surgical management consists in the ligation of the affected vessel proximally and distally to the lesion. Conversely, in more peripherally located lesions (mid to distal superior mesenteric artery) and in end organ perfusion vessels (proper hepatic artery, renal artery), the goal of treatment is an arterial bypass formation preserving distal blood flow, due to the lack of collateral network6.
CΑSE REPORT
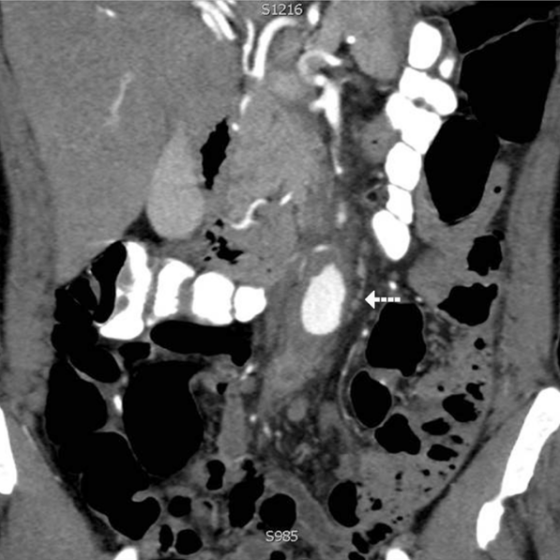
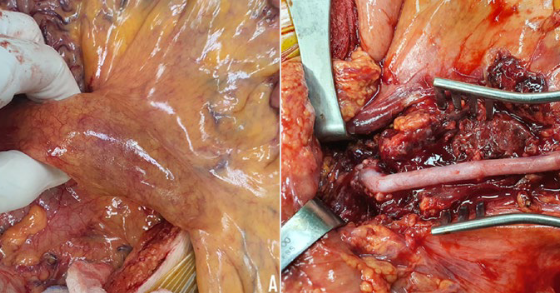
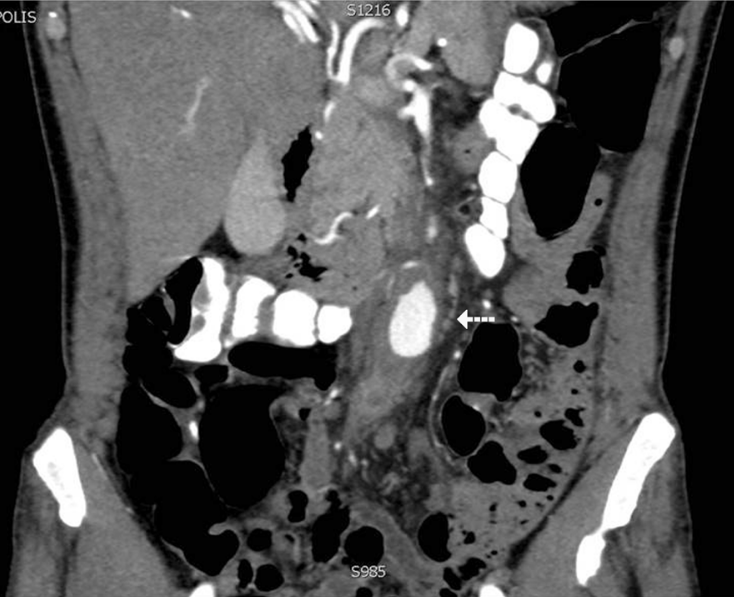
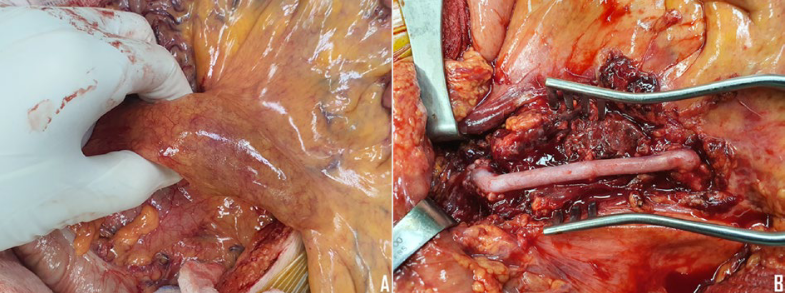
We present the case of a 50-year-old male admitted to our department, suffering from vague abdominal pain for 2 months, due to a recently diagnosed ~28mm in diameter partially thrombosed mycotic pseudoaneurysm of the distal superior mesenteric artery (SMA), originating from infective endocarditis. Transthoracic echocardiography revealed vegetation on the aortic valve, with moderate regurgitation. The source of the pain was confirmed to arise from the infected pseudoaneurysm embolizing the distal arterial collateral network, as depicted in the computed tomography scan of the abdomen (Fig’s. 1 & 2). Abrupt abdominal pain necessitated emergent repair in addition to broad-spectrum antibiotics. After surgical transabdominal intervention, the pulsatile SMA aneurysm was easily recognized (Fig. 3A). Careful dissection of the aneurysm and all patent branches (right colic, ileocolic, lowest jejunal and vasa recta for small bowel) was performed. Caution was applied to preserve the intestinal vascular arcades. Open surgical repair using the great saphenous vein was performed to maintain vascular continuum (Fig. 3B). All available SMA branches emerging from both SMA stumps were incorporated in the proximal and distal anastomosis (Fig. 2). In addition to vascular reconstruction, we inserted the omentum above the sutured aneurysm sac to further protect the vein bypass.
DISCUSSION
According to recent guidelines, endovascular first line option is highly recommended for any SMA aneurysm, independent of the diameter, if anatomically feasible7. However, endovascular stent-grafting was not performed because of the risk of losing those branches emerging from the required healthy sealing zones. Additionally, transcatheter embolization poses the risk of distal branch loss from possible dissemination of coils. Reversal of pain suggested that including the right colic/ ileocolic arteries and the lowest jejunal branch in the proximal anastomosis and two vasa recta in the distal anastomosis, not only intestinal viability was preserved but also collateral circulation improved. Unlike others choosing the femoral vein8, we used a reversed segment of the great saphenous vein because of better size matching with the SMA stumps. However, in the context of an infected field, both autologous great saphenous or femoral vein are appropriate for in situ arterial reconstruction, as they have been associated with advantages8.
Patient course was uneventful. Two weeks later the patient underwent successful aortic valve replacement. A follow-up examination at 3 years founds the patient asymptomatic. In experienced hands, open repair of distally located symptomatic SMA aneurysm is feasible and safe. Preserving arterial continuity in a hostile environment (distal location of the aneurysm, vascular wall inflammation) while salvaging arterial mesenteric branches in close proximity to the aneurysm becomes technically challenging but constitutes the sine qua non for minimizing the risk of enteric ischemia.
REFERENCES
- Matray L, Roisin S, Sabbagh C. Arterial revascularization following acute mesenteric ischemia. J Visc Surg 2020;157:53-8.
- Ferrero E, Ferri M, Viazzo A, Robaldo A, Carbonatto P, Pecchio A, et Visceral artery aneurysms, an experience on 32 cases in a single center: treatment from surgery to multilayer stent. Ann Vasc Surg 2011;25:923-35.
- Cordova AC, Sumpio BE. Visceral Artery Aneurysms and Pseudoaneurysms—Should They All be Managed by Endovascular Techniques? Ann Vasc Dis 2013;6:687-93.
- Borghese O, Ganimede MP, Briatico Vangosa A, Pisani A, Vidali S, Di Stasi C, et al. The Minimally Invasive Treatment of Visceral Artery Pseudoaneurysms: A Retrospective Observational Single Centre Cohort Study on Glue Embolization. Vasc Endovascular Surg 2021 Jul 14:15385744211028730.
- Dohan A, Eveno C, Dautry R, Guerrache Y, Camus M, Boudiaf M, et Role and Effectiveness of Percutaneous Arterial Embolization in Hemodynamically Unstable Patients with Ruptured Splanchnic Artery Pseudoaneurysms. Cardiovasc Intervent Radiol 2015;38:862-70.
- Marone EM, Mascia D, Kahlberg A, Brioschi C, Tshomba Y, Chiesa R. Is open repair still the gold standard in visceral artery aneurysm management? Ann Vasc Surg 2011;25:936-46.
- Chaer RA, Abularrage CJ, Coleman DM, Eslami MH, Kashyap VS, Rockman C, et The Society for Vascular Surgery clinical practice guidelines on the management of visceral aneurysms. J Vasc Surg 2020;72(1S):3S-39S.
- Namkoong M, Hong SB, Kim HW, Jo KH, Kim Open Surgical Repair Using the Femoral Vein for a Mycotic Superior Mesenteric Artery Aneurysm. Korean J Thorac Cardiovasc Surg. 2018;51:209-12.

{kind=link}
{kind=link}
{kind=link}