Endovascular treatment of pulmonary embolism: a systematic review

| Available Online: | October, 2025 |
| Page: | 153–157 |
Author for correspondence:
Ioannis Theodosopoulos
1st Department of Vascular Surgery, Attikon University Hospital, Athens, Greece
E-mail: itheod88@gmail.com
doi: 10.59037/f460yt04
ISSN 2732-7175 / 2025 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Ioannis T. Theodosopoulos, Estelle Ioannidou, Georgios Plakas, Aristotelis Yfantis, John D. Kakisis, Constantine N. Antonopoulos
1st Department of Vascular Surgery, Medical School, National and Kapodistrian University of Athens, Attikon University Hospital, Athens, Greece
Full Text
Gallery
Full Text
Abstract:
Objective: Pulmonary embolism (PE) is a serious cardiopulmonary condition associated with considerable morbidity and mortality, particularly among high-risk patients. The standard therapeutic approach relies on anticoagulation and, in selected cases, systemic thrombolysis. However, these strategies are accompanied by an increased risk of bleeding and may not always achieve rapid restoration of hemodynamic stability. The aim of this study is to conduct a systematic review of the international literature on endovascular techniques in the management of PE, with a focus on mechanical thrombectomy, catheter-directed thrombolysis, and the latest thrombectomy devices (e.g., FlowTriever, Indigo).
Methods: A comprehensive search was performed in PubMed and Google Scholar databases up to October 1st, 2025, to identify relevant studies. The analysis emphasizes effectiveness, safety, complications, and limitations of the available data, while also reviewing current guideline recommendations.
Results: The analysis of 11 studies (RCTs, prospective trials, and registries) demonstrated that endovascular techniques, including ultrasound-assisted thrombolysis (EKOS) and mechanical or pharmacomechanical thrombectomy (FlowTriever, Indigo), achieve rapid and significant improvement in RV/LV ratio and hemodynamic stabilization. In 9 out of 11 studies that used the RV/LV change as an endpoint, the results were particularly encouraging with a mean overall reduction of 0.389. Rates of major bleeding were lower compared with systemic thrombolysis in 8 out of 11 studies (mean rate 2.2%), and overall mortality remained low in most series. In one study (with a significant number of patients, n=800), it was reported that in 87.4% of patients who underwent percutaneous thrombectomy, oxygen requirements decreased within 48h and the percentage of patients with satisfactory oxygen saturation on room air increased from 10.5% to 71.2% postoperatively. However, the available evidence is mainly derived from non-randomized studies and registries, with limited clinical endpoints.
Conclusion: Endovascular techniques appear highly promising, achieving improvement in right ventricular function and hemodynamic stability with a lower risk of bleeding compared to systemic thrombolysis. Nevertheless, the lack of large randomized controlled trials limits the strength of the available evidence. The study highlights the need for further research and the integration of multidisciplinary Pulmonary Embolism Response Teams (PERT) into routine clinical prac-tice.
INTRODUCTION
Pulmonary embolism (PE) remains a leading cause of cardio-vascular morbidity and mortality worldwide, with an estimat-ed annual incidence of 60-70 cases per 100,000 population1. It results from the obstruction of the pulmonary arteries by embolic material—most commonly thrombus—originating from the deep venous system of the lower extremities. The clinical spectrum ranges from mild dyspnea to hemodynamic collapse and sudden death, underscoring the importance of prompt diagnosis and appropriate management.
Anticoagulation remains the cornerstone of therapy, pre-venting thrombus propagation and facilitating endogenous fibrinolysis. In high-risk or massive PE, systemic thrombolysis can rapidly restore pulmonary perfusion but carries a consid-erable risk of major bleeding and is often contraindicated. Sur-gical embolectomy, although effective, is invasive and availa-ble only in specialized centers. These limitations have created a therapeutic gap that has spurred the development of mini-mally invasive endovascular approaches.
Over the past two decades, endovascular therapies have emerged as a promising alternative or adjunct to conventional treatment. Techniques such as catheter-directed thrombolysis (CDT), ultrasound-assisted CDT, pharmacomechanical inter-ventions, and mechanical thrombectomy aim to achieve rapid thrombus reduction, relieve right ventricular (RV) strain, and restore pulmonary hemodynamics while minimizing systemic exposure to thrombolytic agents. New-generation devices like FlowTriever™ and Indigo™ have further expanded the scope of these interventions by enabling single-session mechanical thrombectomy without the need for thrombolytics.
Growing evidence from prospective trials and registries suggests that endovascular therapies offer significant hemo-dynamic improvement with lower bleeding risk compared to systemic thrombolysis2,3. Consequently, major societies —including the European Society of Cardiology (ESC) and the American Heart Association (AHA)—now recognize their role in selected highor intermediate-risk patients, particu-larly when thrombolysis is contraindicated or ineffective4,5. Furthermore, the multidisciplinary Pulmonary Embolism Re-sponse Team (PERT) model has facilitated timely patient selec-tion and improved outcomes6.
This systematic review aims to summarize and critically evaluate the current evidence regarding endovascular treat-ment of acute pulmonary embolism, including the efficacy, safety, and clinical outcomes of available techniques, as well as existing gaps in knowledge and directions for future re-search.
METHODS
This study was designed as a systematic review of the litera-ture following the PRISMA 2020 (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. The objective was to systematically identify, select, and evalu-ate clinical studies addressing endovascular management of acute pulmonary embolism (PE).
Search Strategy
The systematic search was conducted in accordance with PRISMA recommendations. As this work forms part of a post-graduate thesis, no protocol was registered in PROSPERO. A structured search strategy was developed, and the PubMed and Google Scholar databases were explored up to October 1, 2025, to identify studies evaluating endovascular interven-tions for PE. Interventions of interest included catheter-di-rected thrombolysis (CDT), ultrasound-assisted thrombolysis (EKOS), and mechanical thrombectomy using devices such as FlowTriever and Indigo. Reference lists of all included studies were also screened manually for additional eligible publica-tions.
The search strategy combined free-text terms and MeSH headings as follows:
(“Pulmonary Embolism”[Mesh] OR “pulmonary embo-lism” OR “pulmonary thromboembolism”) AND (“Endovascular Procedures”[Mesh] OR “endovascular treatment” OR “endovascular management” OR “catheter-di-rected therapy” OR “catheter-directed thrombolysis” OR “per-cutaneous thrombectomy” OR “interventional radiology”) AND (“mechanical thrombectomy” OR “aspiration thrombectomy” OR “EKOS” OR “FlowTriever” OR “Indigo”).
Inclusion Criteria
Study selection was based on the PICO framework (Popula-tion, Intervention, Comparison, Outcome). Eligible studies included peer-reviewed clinical investigations (randomized controlled trials, prospective and retrospective cohorts, and registries) enrolling adult patients (≥18 years) with acute in-termediateor high-risk PE treated with endovascular tech-niques. Interventions included CDT, ultrasound-assisted CDT (EKOS), and mechanical or pharmacomechanical thrombecto-my (FlowTriever, Indigo).
Outcomes of interest comprised hemodynamic improve-ment (e.g., RV/LV ratio, mean pulmonary artery pressure) and clinical outcomes (mortality, major bleeding, procedural success). Only studies with ≥50 participants and published be-tween 2000-2025 in English were included.
Exclusion Criteria
Exclusion criteria were:
- Case reports or series with <10 patients
- Animal or in vitro studies
- Narrative reviews, expert opinions, or editorials
- Articles lacking full-text data
- Duplicate publications
Study Selection
All retrieved citations were merged and screened for relevance by title and abstract. Irrelevant or duplicate records were ex-cluded. Full texts of potentially eligible articles were reviewed, and those meeting the inclusion criteria were retained.
From an initial 414 unique studies, after duplicate removal and screening, 63 full-text articles were assessed. Of these, 11 studies met all criteria and were included in this systematic review (e.g., ULTIMA, FLARE, FLASH, EXTRACT-PE, EKOS-PE).
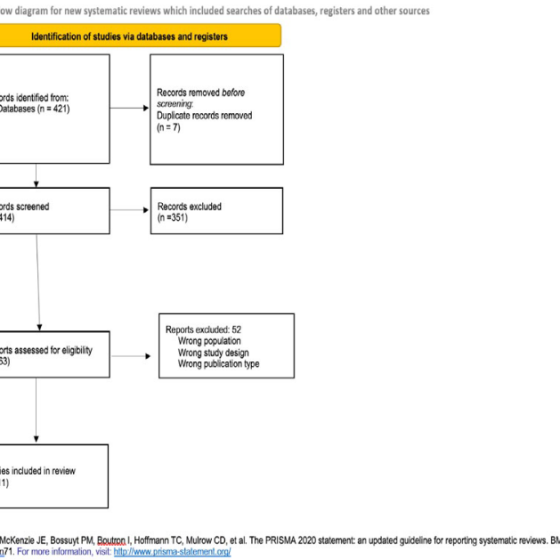
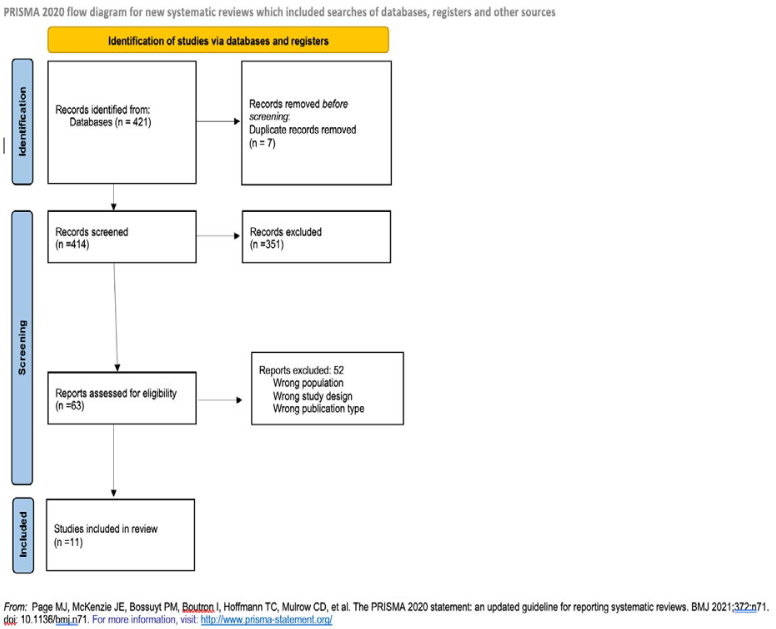
The selection process is summarized in the PRISMA flow diagram (Figure 1).
Data Extraction
From each study, the following information was extracted: first author, publication year, country or study center, sample size, patient characteristics, type of endovascular intervention (CDT, EKOS, FlowTriever, Indigo), and key outcomes such as hemodynamic improvement, complication rates, major bleed-ing, and mortality. Data were organized into a summary table for comparison.
Data Synthesis
Given the heterogeneity of study designs and limited number of randomized controlled trials, no meta-analysis was per-formed. Results are presented descriptively in narrative and tabular form.
RESULTS
The database search yielded 421 publications. After removal of duplicates (n = 7), 414 records were screened. A total of 63 full-text studies were reviewed, and 11 met all inclusion criteria. These comprised randomized trials, prospective mul-ticenter studies, retrospective cohorts, and registries.
Key Findings
- Ultrasound-assisted CDT (EKOS) studies (ULTIMA, SE-ATTLE II, OPTALYSE) consistently demonstrated signif-icant reductions in RV/LV ratio within 24-48 hours, with major bleeding rates <5% and no intracranial
Table 1 Studies included in systematic review
| STUDY | YEAR | METHOD USED | N | TYPE OF STUDY | MAIN OUTCOMES |
| ULTIMA trial – Kucher et al., Circulation7 | 2014 | EKOS (US-CDT) | 59 | RCT (CDT+AC vs AC) | RV/LV ratio reduction (0.30 vs 0.03), no major bleeding |
| SEATTLE II – Piazza et al., JACC:
Cardiovasc Interv8 |
2015 | EKOS | 150 | Prospective multicenter | RV/LV 1.55→1.13. Major bleeding 10%, no ICH |
| OPTALYSE PE – Tapson et al., JACC9 | 2018 | EKOS (dose-ranging) | 101 | Prospective multicenter | RV/LV -0.3 to -0.4 with low dose tPA, bleeding <4% |
| SUNSET sPE – Avgerinos et al., Circulation10 | 2021 | EKOS vs CDT | 82 | RCT | No difference in clot burden, RV/LV improved, safe |
| FLARE trial – Tu et al., JACC:
Cardiovasc Interv11 |
2019 | FlowTriever | 106 | Prospective multicenter | RV/LV 1.53→1.15. 0% ICH,
mortality 1% |
| FLASH registry – Toma et al., JACC12 | 2022 | FlowTriever | >800 | Real-world registry | Hemodynamic improvement,
mortality 0.8%, bleeding <2% |
| EXTRACT-PE – Sista et al., JACC13 | 2021 | Indigo | 119 | Prospective multicenter | RV/LV 1.47→1.04. Bleeding 1.7%, no ICH |
| Indigo multi-center study – Sylwia Sławek-Szmyt et al., JACC3 | 2023 | Indigo | 110 | Multicenter prospective registry | RV/LV 0.48 benefit, bleeding low, procedural success >90% |
| PERFECT registry – Kuo et al., Chest14 | 2015 | CDT & MT | 101 | Multicenter registry | Clinical success 86%, mortality 4%, no ICH |
| FLARE ED substudy – Jaber et al., JACC15 | 2023 | FlowTriever | ~100 | Prospective substudy | Rapid stabilization, RV/LV improved, 0% ICH |
| PERT Consortium – Kattih et al., JACC6 | 2020-22 | Mixed | ~200–300 | Registry | Mortality 2–4%, outcomes consistent |
- Mechanical thrombectomy with FlowTriever (FLARE trial, FLASH registry) showed rapid hemodynamic improvement, mortality <1%, and minimal bleeding risk.
- Aspiration thrombectomy using the Indigo system (EXTRACT-PE trial, Indigo registry) achieved marked reductions in RV/LV ratio with major bleeding <2%.
- Large multicenter registries (PERFECT, PERT Consorti-um, FLASH) confirmed high procedural success (>85%) and low periprocedural mortality (2-4%) in real-world
- Across studies, endovascular therapies achieved a mean RV/LV reduction of 0.39 and an average ma-jor bleeding rate of 2.2%. In one large registry (>800 patients), oxygen requirements decreased markedly within 48 hours, with the proportion of patients main-taining room-air saturation rising from 5% pre-pro-cedure to 71.2% post-procedure.
Collectively, these data suggest that endovascular inter-ventions rapidly restore hemodynamics and right ventricular function while minimizing hemorrhagic complications com-pared to systemic thrombolysis.
Ultrasound-Assisted Thrombolysis (EKOS)
ULTIMA (2014): RCT (n=59); RV/LV ratio decreased 1.28→0.99 (-23%); no major or intracranial bleeding; 0% mortality.
SEATTLE II (2015): Prospective multicenter study (n=150); RV/ LV 1.55→1.13 in 48h; 10% major bleeding, no ICH; improved mPAP and cardiac index.
OPTALYSE-PE (2018): Multicenter (n=101); low-dose tPA (4-12 mg) infusions over 2-6h reduced RV/LV by 0.3-0.4; <4% major bleeding.
SUNSET sPE (2021): RCT (n=82); EKOS vs standard CDT; sim-ilar thrombus resolution and RV/LV improvement; no safety difference.
Mechanical Thrombectomy FlowTriever
FLARE (2019): Prospective (n=106); RV/LV 1.53→1.15 in 48h; no ICH, minimal bleeding.
FLASH Registry (2022): >800 patients; reduced mPAP, im-proved cardiac output; 30-day mortality 0.8%, major bleeding <2%.
FLARE-ED (2023): Emergency department substudy; confirmed rapid RV/LV improvement and hemodynamic stabiliza-tion; 0% ICH.
Aspiration Thrombectomy Indigo
EXTRACT-PE (2021): Prospective (n=119); RV/LV 1.47→1.04 in 48h; 1.7% major bleeding, no ICH.
Indigo Registry (2023): 110 patients; procedural success >90%, low complication rate.
COMBINED TECHNIQUES AND REGISTRIES
PERFECT Registry (2015): Multicenter CDT & mechanical thrombectomy (n=101); clinical success 86%, mortality ~4%, no ICH.
PERT Consortium Data (2020-2022): ~200-300 patients; mor-tality 2-4%, good safety profile despite procedural heteroge-neity; highlights multidisciplinary PERT value.
Summary of Findings
Across 11 major studies, endovascular therapies (CDT, EKOS, FlowTriever, Indigo) consistently demonstrated significant hemodynamic and clinical improvement with markedly low-er bleeding risk than systemic thrombolysis. Ultrasound-as-sisted thrombolysis appears safe, though its superiority over standard CDT remains uncertain. Mechanical thrombectomy with FlowTriever and Indigo shows excellent safety and effi-cacy without the need for thrombolytics. Registry data (PER-FECT, FLASH, PERT) strengthen external validity and reflect real-world practice.
However, the lack of large randomized trials and limited long-term follow-up remain major limitations.
DISCUSSION
This systematic review highlights that endovascular therapy represents a highly promising treatment option for acute PE, especially in intermediateand high-risk patients for whom systemic thrombolysis is contraindicated or carries excessive bleeding risk.
EKOS-based studies demonstrate that low-dose local thrombolysis can achieve rapid right ventricular unloading with minimal bleeding complications. Mechanical thrombec-tomy systems such as FlowTriever and Indigo further advance safety by eliminating thrombolytics altogether, providing im-mediate thrombus debulking and hemodynamic stabilization.
Nevertheless, several limitations temper the evidence:
- Most studies were single-arm and lacked control
- The number of large randomized trials remains lim-ited (e.g., ULTIMA, SUNSET sPE), with relatively small
- Follow-up periods were short, with scarce data on chronic outcomes such as CTEPH.
- Outcome heterogeneity (RV/LV ratio, hemodynamic endpoints, mortality, complications) complicates di-rect comparison across studies.
- Reported improvements, though clinically meaning-ful, should be interpreted cautiously due to study var-
Current ESC (2019) and ATS guidelines endorse endovas-cular therapies as alternative options in selected cases but emphasize the need for robust, well-designed randomized trials.
In conclusion, while the existing evidence strongly sup-ports the efficacy and safety of endovascular approaches, their definitive role in the PE treatment algorithm requires further validation through large-scale, long-term randomized studies. The establishment of multidisciplinary Pulmonary Embolism Response Teams (PERTs) is likely to enhance pa-tient selection, streamline decision-making, and improve overall clinical outcomes.
REFERENCES
- Vyas V, Sankari A, Goyal A. Acute Pulmonary Embolism. Published online December 11, Accessed October 8, https://www.ncbi.nlm.nih.gov/books/NBK560551/
- Toma C, Jaber WA, Weinberg MD, et al. Acute outcomes for the full US cohort of the FLASH mechanical thrombec-tomy registry in pulmonary embolism. EuroIntervention. 2023;18(14):1201-1212. doi:10.4244/EIJ-D-22-00732
- Sista AK Horowitz JM TVFRMEMDSBJDSANEDD, Inves-tigators. E-P. Indigo Aspiration System for Treatment of Pulmonary Embolism: Results of the EXTRACT-PE Trial. doi:10.1016/j.jcin.2020.09.053
- Takahashi EA, Sista AK, Addison D, et Disparities in Cur-rent Pulmonary Embolism Management and Outcomes: A Scientific Statement From the American Heart Asso-ciation. Circulation. 2025;151(15):e944. doi:10.1161/ CIR.0000000000001306
- Konstantinides S V., Meyer G, Bueno H, et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European respiratory society (ERS). Eur Heart J. 2020;41(4):543-603. doi:10.1093/EURHEARTJ/EHZ405
- Kattih Z Meredith S RVDVVASATSLTKAKC. Mechanical thrombectomy vs catheter directed thrombolysis vs anti-coagulation alone: A tertiary center PERT Registry Cohort Analysis. doi:10.1016/j.thromres.2024.109114
- Kucher N, Boekstegers P, Müller OJ, et al. Randomized, controlled trial of ultrasound-assisted catheter-directed thrombolysis for acute intermediate-risk pulmonary em-bolism. Circulation. 2014;129(4):479-486. doi:10.1161/ 113.005544
- Piazza G Hohlfelder B ., Investigators. SII. A Prospective, Single-Arm, Multicenter Trial of Ultrasound-Facilitated, Catheter-Directed, Low-Dose Fibrinolysis for Acute Massive and Submassive Pulmo-nary Embolism: The SEATTLE II Study. doi:10.1016/j. jcin.2015.04.020
- Tapson VF, Sterling K, Jones N, et al. A Randomized Trial of the Optimum Duration of Acoustic Pulse Thromboly-sis Procedure in Acute Intermediate-Risk Pulmonary Em-bolism: The OPTALYSE PE Trial. JACC Cardiovasc Interv. 2018;11(14):1401-1410. doi:10.1016/J.JCIN.2018.04.008
- Avgerinos ED Jaber W LJMKMMR-LBNRCBSJT. ., sPE Col-laborators. Randomized Trial Comparing Standard Ver-sus Ultrasound-Assisted Thrombolysis for Submassive Pul-monary Embolism: The SUNSET sPE Trial. doi:10.1016/j. jcin.2021.04.049
- Tu T Toma C TVFACJWASMKSARWME, Investigators. F. A Prospective, Single-Arm, Multicenter Trial of Cathe-ter-Directed Mechanical Thrombectomy for Intermedi-ate-Risk Acute Pulmonary Embolism: The FLARE Study. doi:10.1016/j.jcin.2018.12.022
- Toma C Jaber WA WMDBMCKSSBGSCJARL. . Acute out-comes for the full US cohort of the FLASH mechani-cal thrombectomy registry in pulmonary embolism. doi:10.4244/EIJ-D-22-00732
- Sista AK, Horowitz JM, Tapson VF, et Indigo Aspiration System for Treatment of Pulmonary Embolism: Results of the EXTRACT-PE Trial. Cardiovasc Interv. 2021;14(3):319-doi:10.1016/J.JCIN.2020.09.053
- Kuo WT, Banerjee A, Kim PS, et al. Pulmonary Embolism Response to Fragmentation, Embolectomy, and Catheter Thrombolysis (PERFECT): Initial Results From a Prospec-tive Multicenter Registry. Chest. 2015;148(3):667-673. doi:10.1378/CHEST.15-0119
- Jaber WA Kabrhel C Percutaneous Thrombec-tomy in Emergency Department Patients with Pulmo-nary Embolism: The FLARE ED Sub-study. doi:10.1016/j. jemermed.2019.11.044
{kind=link}