European Junior Doctors’ Work Experiences, Job Satisfaction, and Proposals for Reform – with Contextual Emphasis on Greece

| Available Online: | March, 2026 |
| Page: | 12–19 |
Author for correspondence:
Konstantinos Roditis
Consultant Vascular Surgeon
Zinonos 32, 15234, Halandri, Greece
E-mail: roditis.k@gmail.com
doi: 10.59037/yxrbpq96
eISSN: 2732-7167 / 2026 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
1 Consultant Vascular Surgeon, Department of Vascular Surgery, Korgialenio-Benakio Hellenic Red Cross Hospital, Athens, Greece
2 Junior Doctors’ Network-Hellas (JDN-Hellas), Athens, Greece
3 European Junior Doctors Association (EJD), Brussels, Belgium
4 1st Department of Obstetrics and Gynecology, Aristotle University of Thessaloniki, General Hospital Papageorgiou, Thessaloniki, Greece
5 Department of Pediatrics, General Hospital of Volos
6 Department of ENT, Panarkadiko General Hospital, Tripoli, Greece
7 1st Department of Propaedeutic Surgery, Hippokration General Hospital, Medical School, National and Kapodistrian University of Athens, Greece
8 3rd Surgical Department, Euroclinic Athens, Greece
Full Text
Gallery
Full Text
Abstract:
Introduction: Despite workforce growth, European healthcare systems face ongoing shortages, uneven distribution, and retention challenges, all worsened by COVID-19. Nearly half of residents experience burnout, driven by workload, poor environments, and rigidity. In Greece, the pandemic deepened exhaustion, burnout, and distrust in the health system, as shown by the JDN-Hellas/PhMA “Barometer” findings. Vascular trainees were also affected, reporting steep declines in operative exposure and confidence – reflecting the broader European crisis in postgraduate training and the need for targeted retention strategies.
Methods: The present study’s purpose is to review the results of a pan-European qualitative study conducted by the European Junior Doctors Association (EJD) to explore the work-related experiences of junior doctors (JD) and their impact on professional and personal wellbeing. Between January and June 2023, 25 representatives were interviewed (10 men, 15 women) from 24 EJD member countries. Seventeen interviews were held in English via online platforms. Transcripts were analysed using ATLAS.ti v9. Sampling was purposive, ensuring gender representation. Ethical approval and informed consent were obtained in accordance with the EU General Data Protection Regulation (GDPR).
Results: Despite contextual diversity, the participants demonstrated a notable agreement on the principal challenges. Across Europe, dissatisfaction, exhaustion, frustration, and insecurity stem from challenging working conditions, excessive workload, long and unpredictable hours, and inflexibility. Workload demands and a lack of resources negatively impact both learning and quality of care, consequently fueling stress and burnout. Deficiencies in supervision, time allocation, and feedback compromise training quality. Inequalities related to gender and migration, including obstacles like career breaks, negative perception of part-time work, blocked career advancement, and limited possibilities, exacerbate susceptibility. Changes in values across generations, emphasizing work-life balance and self-care, are causing both job departures and shifts in career choices. Nordic countries demonstrate superior practices through adaptable scheduling and robust equity policies.
Conclusion: Junior doctors’ dissatisfaction threatens workforce sustainability. Improving retention necessitates integrated European and national strategies that prioritise flexibility, safe staffing levels, fair remuneration, protected training opportunities, and equity. Within Greece, where burnout and distrust persist, the implementation of such reforms and the fostering of institutional transparency are essential to restoring morale and protecting healthcare resilience.
Keywords: junior doctors, workforce retention, burnout, work–life balance, job satisfaction
INTRODUCTION
1. Background
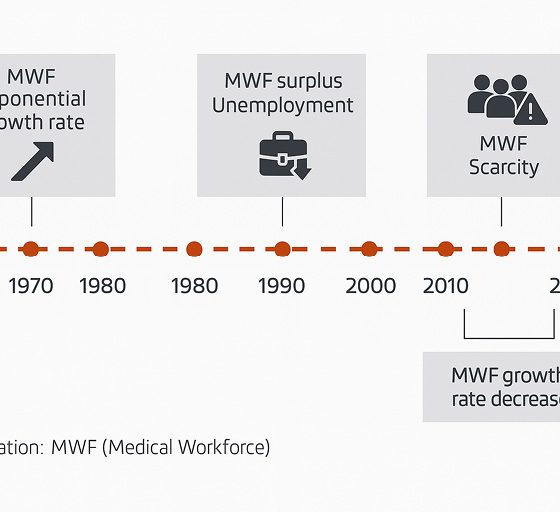
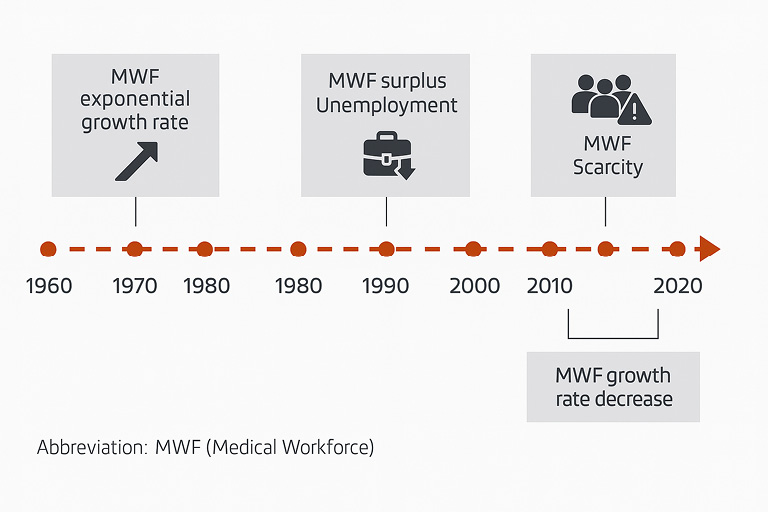
Since the 1960s, the European Union has seen sustained growth in its health workforce, including physicians, driven by demographic ageing and demand-side trends in convenience-oriented care delivery. Despite this growth, all countries in the WHO European Region face intensifying medical workforce (MWF) planning challenges (Figure 1) – long-term shortages, maldistribution (e.g., rural/remote “medical deserts”), recruitment deficits in key sectors (primary care, mental health), and underinvestment in workforce development – exacerbated by the COVID-19 pandemic’s system shocks.1-3 Retention has thus moved to the forefront of MWF planning: job dissatisfaction is strongly associated with intentions to quit (Mobley’s model), while negative self-evaluation and poor work experiences are linked to psychological distress and burnout.4-7 Junior doctors (JD) are particularly vulnerable; meta-analytic estimates suggest nearly half of residents experience burnout, with work-related drivers (workload, patient-care stressors, poor environments, work-life imbalance) outweighing nonmodifiable factors.8-10 EJD’s 2022 survey already highlighted work overload and career “bottlenecks” across transitions.11
Simultaneously, the profession’s demographics are changing: the workforce is aging (approximately 30% over 60 years old in Europe, near-term retirements) and becoming increasingly feminized (women from 43% in 2010 to 48% in 2020), while gender inequities persist (approximately 20% health-sector pay gap, under-representation in leadership), with female gender identified as a risk factor for burnout in young doctors.2,10,12,13
2. Situation in Greece
The situation in Greece encapsulates many of the pressures described across Europe but with amplified intensity. Years of underinvestment, low remuneration and rigid administrative structures have created a system that relies heavenly on personal dedication rather than institutional support. Junior doctors often rotate through understaffed regional hospitals with long on-call stretches -that go beyond the official maximum working hours directive, with average weekly hours 65± and limited supervision, while mandatory service obligations delay career planning and family life. These conditions, combined with low perceived transparency and minimal feedback loops, have eroded professional trust and contributed to a long-standing outward migration of doctors putting additional strain on the remaining staff. During the pandemic, Greek physicians reported marked exhaustion and rising burnout, with public discourse highlighting systemic strain and entrenched distrust toward health institutions.14-16
The initial findings from the JDN-Hellas / Panhellenic Medical Association (PhMA) “Barometer” of Greek junior doctors mirror the European trends of exhaustion and dissatisfaction but reveal a deeper cultural dimension: a sense of powerlessness and detachment from decision-making. This, along with the perception of a significant workload, inadequate support, dissatisfaction with the national healthcare system, and regular exhaustion, indicated that technical reforms alone (e.g., salary adjustments) will not suffice without parallel measures. It highlights the pressing need for Greek-tailored policy adjustments that will rebuild confidence in institutions and governance.17 Greece represents a microcosm of the wider European crisis, illustrating what happens when workforce fragility meets structural rigidity.
3. Vascular trainees after COVID-19
Among all medical disciplines, procedural and emergency specialties -particularly surgical specialties- demonstrate the most acute interaction between workload, supervision and training quality. In such environments, extended hours and unpredictable emergencies directly affect patient safety and skill acquisition. Vascular surgery exemplifies this tension: the field combines technical precision with high emergency burden, making consistent operative exposure and mentoring essential for competence. When service pressure rises and elective caseloads fall, as during COVID-19, trainees lose both confidence and progression milestones. These challenges are not unique to surgery but act as a magnifying lens for how systemic inefficiencies translate into training deficits and burnout across the profession. A European survey by Pereira-Neves et al. (2022) showed that nearly 77% of vascular trainees experienced reduced operative exposure during the COVID-19 pandemic, and 60% reported a decline greater than half. Over 70% felt their training and career progression were negatively affected, and almost half of senior trainees faced fewer job prospects. Despite online teaching efforts, most called for compensatory measures to offset lost experience. These findings highlight how pandemic disruptions worsened workload, limited training, and deepened uncertainty – mirroring challenges faced by junior doctors across Europe, including Greece.18
To address these gaps, the EVaST (European Vascular Surgical Training) Survey, led by the ESVS and EVST, will collect Europe-wide data on training, simulation, and mentorship. Through anonymised feedback from trainees and trainers, EVaST aims to identify effective educational models and expose disparities. The initiative seeks to build a unified, data-driven foundation for improving vascular training quality, fostering mentorship, and ensuring the next generation of vascular surgeons is both technically skilled and professionally supported.19
4. Study rationale
Understanding JD work experiences and their impacts is essential to inform retention-oriented reforms. This paper presents the qualitative findings of EJD’s pan-European study 20 and synthesizes proposals from JD representatives, with specific attention to Greece.
5. Objectives
General objective: To explore European junior doctors’ work-related experiences and the impact of those experiences on their professional and personal lives.
Specific objectives: a) To identify commonalities in JD work-related experiences across the EJD’s member countries, b) to collect proposals from JD to increase job satisfaction and contribute to retention in this group.
METHODS
1. Methodology
The present study is based on the results of a pan-European qualitative study20 which employed semi-structured interviews and thematic analysis (ATLAS.ti v9). This study was conducted by EJD between January and June 2023 with representatives from EJD national member associations. Purposive sampling of EJD-nominated country representatives (close to the research problem, representing national JD). Gender balancing achieved (parity or female over-representation). N=25 participants (10 men, 15 women), ages 25-47; 16 in postgraduate training (PGT) and 9 early career specialists (ECS). Seventeen interviews were held (8 dyads, 9 individuals). To deepen the analysis of gender inequities, an additional group comprising women from contexts with advanced gender-equity measures was convened (Finland, with double representation). Sociodemographic data of participants are shown in detail in Table 1.
2. Data collection and analysis
Interviews (English, online; ≈90 minutes for dyads, ≈60 minutes individual) followed a consensual guide but allowed flexibility to elicit diverse perspectives. Interviews were audio-recorded with consent. Dimensions probed included job satisfaction, wellbeing, resignations, work experiences, training quality, personal life affects, gender inequalities, proposals, and context-specific issues (Table 2). Thematic analysis of interview transcripts was conducted to identify recurrent patterns and categories reflecting European junior doctors’ shared experiences. The analysis was performed using ATLAS.ti v9 (Scientific Software Development GmbH, Berlin, Germany). This software facilitates a transparent and systematic approach to qualitative analysis. Informed consent obtained. Personal data processed under EU GDPR (Regulation 2016/679). To protect confidentiality, quotes are not linked to identifiable country data (Turkey excepted due to unique context). A list of organizations providing representatives is available by the study’s authors upon request.
RESULTS
Heterogeneity across European systems (financing, organization, training, remuneration, culture) coexists with high cross-national consensus among JD on core concerns. We summarize (i) an overview of JD situations (feelings, vulnerabilities, generational shift, resignations), (ii) factors shaping job satisfaction (work, training, overload, inequities), and (iii) proposals.
1. Overview of European junior doctors’ situation
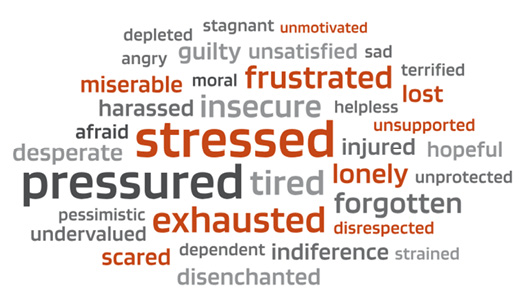
JDs are motivated and enthusiastic, yet report pervasive negative emotions: tiredness/exhaustion, frustration, insecurity, stress, and pressure. Psychological distress is frequently mentioned, including anxiety, depression, burnout, and even suicidal ideation (Figure 2). Two structural vulnerabilities recur:
- Dependence on mentors (dual roles as supervisors and evaluators), which constrains voice and raises fear of repercussions regarding workload, schedules, and leave.
- Limited experience in high-pressure, high-responsibility environments (especially post-COVID), with abrupt entry and insufficient monitoring of mental-health impact; the transition to specialist roles can be sudden, with responsibility outpacing support.

Figure 2. Word cloud: Emotions and feelings of junior doctors
1.1. The generational change regarding work
Participants consistently describe a value shift: today’s JD prize work-life balance, protected time, and fair compensation over “total vocational sacrifice.” They increasingly set boundaries (e.g., on unsafe overtime) and seek flexibility (e.g., scheduling, academic time). Workforce shortages also confer more agency in job and specialty selection. Feminization has catalyzed cultural change – initially voiced by women, now embraced broadly.
Consequences include specialty choice drift toward domains with predictable hours or fewer on-calls, and declining attractiveness of medicine for some students where conditions are comparatively worse than in other sectors.
With few Nordic exceptions, resignations are reportedly rising – before or after residency – and post-training migration to better conditions is common. Some graduates depart clinical medicine altogether (e.g., pharma, consulting). Drivers include stressful/rigid conditions, inadequate staffing, lack of career continuity (no guaranteed posts), and EU mobility opportunities.
2. Factors that influence European junior doctors’ job satisfaction
Lack of flexibility, overload, long hours, and poor environments degrade satisfaction, learning, and health – most acutely for residents, while early-career specialists face temporariness and location mandates.
2.1. Work-related experiences
Four drivers dominate:
- Lack of flexibility. Hinders academic development, conference participation, and caregiving responsibilities; flexibility is pivotal for modern professional identities.
- Compensation concerns. Pay is often perceived as misaligned with workload/ responsibility; may push JD to extend hours, though salary alone won’t fix dissatisfaction.
- Mobility & temporariness. Frequent relocations during and after PGT, weak career projection, temporary contracts, unclear employment rights (e.g., university vs. labor contracts), and in some contexts mandatory rural service post-residency – fostering instability and isolation.
- Working environment. Persistent tension, pressure, stress; impaired interprofessional relations; low recognition. Some Nordic/Central contexts report positive shifts (support for relocation, training opportunities, greater flexibility).
2.2. Training-related experiences
While many PGT programs are valued, work stress degrades training quality:
- Insufficient time for study and academic activities; training time displaced by bureaucratic/nonmedical tasks.
- Supervision gaps and limited feedback, especially on nights/on-call; limited incentives and time for mentors.
- Competency attainment is harder under overload; variable standards across sites; structural issues (e.g., too many residents for caseloads, too few accredited centers/mentors).
- Resultant insecurity about clinical progress and care quality.
Universally cited and worsening:
- Demand increases without commensurate resource growth generate high pace, hasty decisions, and “firefighting,” with limited time to consult or reflect – fueling moral distress and frustration.
- Overload propagates vicious cycles of fatigue and under-recovery, undermining work-life balance and retention.
- JD shoulder many nonmedical tasks amid staff shortages; their dependent status narrows options to reduce hours or change posts.
- Some systems (notably Nordic) report movement away from perceiving JD as “cheap labour”, with fairer task distribution.
2.4. Working times/EWTD
EWTD has improved conditions in several countries, but compliance varies. Even where observed, postponed rest, excessive hours, and night work remain common, harming wellbeing and learning (especially in procedural and emergency specialties).
2.5. Working environment revisited
Overload plus resource scarcity breeds poor climates (competition, incivility), disproportionately affecting JD; recognition deficits amplify demoralization. Change is uneven; “revanchist” cultures (“we suffered, so must you”) slow progress.
Gendered and migration-related inequities compound JD vulnerability; progress varies, with Nordic/Central contexts reporting stronger public care supports and equity policies.
Gender
Despite feminization, women face:
- Career interruptions for caregiving; more part-time and stigma thereof; reduced opportunities and recognition.
- Glass ceiling and leadership under-representation; specialty segregation (women underrepresented in surgical fields), with greater exposure to harassment in some settings.
- Pay gaps emerge indirectly via interruptions, fewer on-calls, and specialty mix.
Migration
Migrant JD encounter racism/xenophobia, limited training & employment opportunities, language barriers, and social isolation – despite their growing system contribution.
3. Proposals
JD proposals cluster into governance & planning, working conditions & balance, occupational wellbeing, training, and inequalities.
3.1. Governance & planning
- Elevate medical workforce to a top political priority.
- Implement robust planning/forecasting
- Strategically address maldistribution (e.g., incentives for medical deserts)
- Increase health-workforce investment.
- Align policies with evolving work values.
3.2. Working conditions & balance
- Flexibility & autonomy: options for part-time, flexible scheduling, academic/protected time, and facilitated transfers.
- Environment: HR best-practice adoption (civility, teamwork, soft-skills training); reduce bureaucracy through digitalization.
- Workload: monitor and reduce; add staff where needed; attend to high-risk contexts (nights, emergency, procedural specialties).
- Hours & rest: enforce EWTD, monitor time, pay overtime, ensure rest facilities and fatigue-risk management.
- Stability: longer contracts and career planning.
- Pay: fair and adequate remuneration (as part of a bundle, not a stand-alone fix).
3.3. Occupational wellbeing
- Prioritize primary prevention (fix conditions). Expand research/monitoring (prevalence, dashboards).
- Build peer networks and structured debriefing (e.g., Balint groups), on paid time.
- Implement violence prevention protocols and safe leave policies; reasonable accommodations for vulnerable JD.
- Train leaders in mental-health supportive management; embed mental-health literacy in PGT core curricula.
3.4. Training
- Protect structured, competency-based programs via supervisor preparation (including incentives) and protected training time.
- Reduce variability by aligning to European standards; increase accountability through evaluation of residents, mentors, and institutions (at multiple time points).
- Fund and time-protect academic development (courses, conferences, research).
3.5. Inequalities
- Treat parental leave as active time; promote paternity-leave uptake; maintain full-time feasibility via public care services.
- Affirmative actions for leadership parity; pay-gap monitoring and remediation funds; targeted recruitment of women in under-represented specialties.
- System-wide training on gender and diversity; targeted supports for migrant JDs.
3.6. Translation into Policy
Bridging the gap between policy and practice requires translating shared concern into enforceable measures. The findings point toward a coherent policy package: adherence to working time regulations, transparent career progression, structured mentorship and supervision incentives, and the systematic integration of wellbeing and equity into workforce governance. There are not optional welfare measures but prerequisites for patient safety and health system resilience. Pilot initiatives -such as national burnout observatories or flexible rotation frameworks- could serve as scalable models across Europe, particularly in contexts like Greece where trust and retention remain fragile. The synthesis of these proposals sets the stage for the concluding discussion on practical implementation and the broader implications for workforce resilience.
CONCLUSION
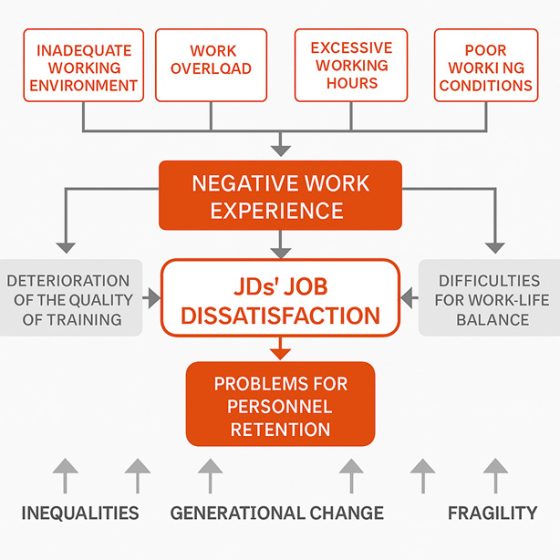
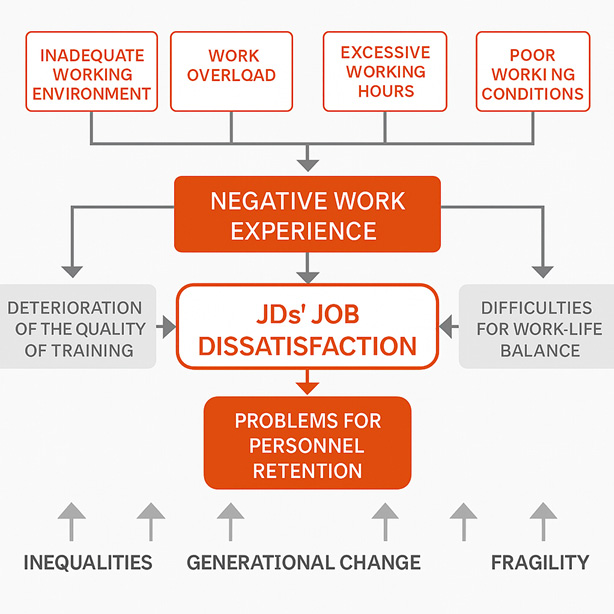
Across Europe, there’s a notable consistency in job satisfaction reports: high workloads, rigid and volatile working conditions, declining training standards, and inequities, all reflecting a generational preference for work-life balance and respectful, safe employment. The combination of these factors negatively affects satisfaction, learning, and retention (Figure 3).
1. Challenges & outlooks for vascular trainees
Procedural specialties, and vascular surgery in particular, have emerged as sentinel indicators of post-pandemic training deficits. Beyond reduced operative numbers, many trainees reported fragmented mentorship, suspended fellowships and redeployment to non-surgical services. The resulting loss of continuity has affected both confidence and retention, with some considering early career change. The Pereira-Neves et al. survey found that over 70% of vascular trainees reported educational regression due to reduced procedures and redeployment. Many expressed concerns about long-term competency and employability. To rebuild competence and morale, training systems should adopt structured compensatory measures, such as simulation-based training, supervised extended fellowships, formalised mentorship networks. Cross-border collaboration—supported by European scientific societies- could equalise opportunities between peripheral and central regions. These measures align with the EJD proposals on flexibility and protected training time but add a specialty-specific dimension: ensuring that technical skill progression keeps pace with service recovery, especially in settings like Greece, where systemic fatigue and limited trust already challenge specialist retention.18, 19
2. Implications for Greece
Greek physicians entered COVID-19 with pre-existing system fragilities; the pandemic accelerated exhaustion, burnout, and distrust toward institutions.14-16 Preliminary “Barometer” findings among Greek JD—high workload, insufficient support, low satisfaction, frequent exhaustion—mirror Europe-wide patterns but appear amplified in Greece.17 Greece should therefore prioritize:
- trust-building measures (transparent governance, participatory decision-making),
- condition-first prevention (staffing, EWTD enforcement, rest, reduced bureaucracy),
- protected training time and supervision,
- stable career pathways and flexibility, and
- equity investments (public childcare, leadership parity initiatives).
Delivering this bundle – not piecemeal fixes – offers the best chance to retain JD, restore morale, and strengthen care quality.
Ensuring the future resilience of European healthcare requires listening to and acting upon the voices of its junior doctors. Their experiences reveal a system under strain but also a clear roadmap for improvement—fair conditions, protected training, meaningful flexibility, and genuine equity. Addressing these needs is not only a matter of workforce sustainability but a commitment to safe, high-quality patient care. By prioritizing wellbeing and modernizing medical workforce policies, Europe can rebuild trust, retain its young clinicians, and secure a stronger, more compassionate health system for the generations to come.
BIBLIOGRAPHY
- Eurostat. Healthcare personnel statistics – physicians. Statistics Explained [Internet]. 2022. [cited 2023 Jul 04]. Available from: https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Healthcare_personnel_statistics_-_physicians&oldid=460643#Healthcare_personnel
- OECD, European Observatory. State of Health in the EU: Companion Report 2021 [Internet]. Luxembourg: Publications Office of the European Union, 2022. Available from: https://ec.europa.eu/health/sites/default/files/state/docs/2019_companion_en.pdf
- WHO Europe Health Workforce and Service Delivery. Health and care workforce in Europe: time to act [Internet]. Copenhagen: WHO Regional Office for Europe; 2022 [cited 2025 Oct 14]. 1-205 p. Available from: https://www.who.int/europe/publications/i/item/9789289058339
- Fragkiadakis GF. The impact of COVID-19 on European and Greek healthcare systems: an overview of public finances and healthcare challenges. ICBE-HOU [Internet]. 2024 Aug. 1 [cited 2025 Oct. 14];3(1). Available from: https://eproceedings.epublishing.ekt.gr/index.php/ICBE-HOU/article/view/7123
- Mobley WH. Intermediate linkages in the relationship between job satisfaction and employee turnover. J Appl Psychol. 1977;62:237-40.
- Hom PW, Griffeth RW, Sellaro CL. The validity of Mobley’s (1977) model of employee turnover. Organ Behav Hum Perform. 1984 Oct;34(2):141-74.
- Maslach C, Schaufeli WB, Leiter MP. Job burnout. Annu Rev Psychol. 2001;52:397-422.
- Klesmite-Bluma A, Cerame A, Berhanu D, Pihelgas P, Eerens D, Trumpickaitė M. On behalf of the European Junior Doctors Association. From mandate to motivation: transforming junior doctors’ retention strategies in Europe [Internet]. Brussels: European Junior Doctors Association; 2024 [cited 2025 Oct 14]. Available at: https://www.juniordoctors.eu/sites/default/files/2024-07/FMM_FINAL.pdf
- Naji L, Singh B, Shah A, Naji F, Dennis B, Kavanagh O, Banfield L, Alyass A, Razak F, Samaan Z, Profetto J, Thabane L, Sohani ZN. Global prevalence of burnout among postgraduate medical trainees: a systematic review and meta-regression. CMAJ Open. 2021 Mar 8;9(1):E189-E200.
- Hariharan TS, Griffin B. A review of the factors related to burnout at the early-career stage of medicine. Med Teach [Internet]. 2019 [cited 2025 Oct 14]; 41(12): 1380-91. Available from: https://www.tandfonline.com/doi/abs/10.1080/0142159X.2019.1641189?journalCode=imte20
- Zhou AY, Panagioti M, Esmail A, Agius R, Van Tongeren M, Bower P. Factors Associated With Burnout and Stress in Trainee Physicians. JAMA Netw Open [Internet]. 2020 [cited 2025 Oct 14]; 18;3(8):e2013761. Available from: https://jamanetwork.com/journals/jamanetworkopen/fullarticle/2769385
- Cerame, A. On behalf of the European Junior Doctors Association. Medical Workforce Planning in Europe: Overview and 2022 preliminary survey’s results. European Junior Doctors Association; 2022. Internal report.
- WHO and the International Labour Organization. The gender pay gap in the health and care sector a global analysis in the time of COVID-19. Geneva: World Health Organization. [Internet]. [cited 2025 Oct 14]. Available from: https://www.who.int/publications/i/item/9789240052895
- Georganta M-N. The pandemic has exhausted doctors in Europe [Internet]. Athens: Eleftheros Typos Newspaper; 15 Nov 2022 [cited 2025 Oct 14]. Available at: https://eleftherostypos.gr/ygeia-epistimi/i-pandimia-exantlise-tous-giatrous-stin-evropi
- Ignatiadis V. How much were doctors’ burnout rates increased in the pandemic [Internet]? Athens: Iatronet online health newspaper; 9 Dec 2023 [cited 2025 Oct 14]. Available at: https://www.iatronet.gr/article/121226/poso-ayxhthhke-to-burnout-ton-giatron-sthn-pandhmia
- Papadatos-Anagnostopoulos D. Who and why don’t trust the healthcare system and why this is a serious problem [Internet]. Athens: Ygeianet online health portal; 16 Sep 2025 [cited 2025 Oct 14]. Available at: https://ygeianet.gr/poioi-kai-giati-den-empisteyontai-to-systima-ygeias-kai-giati-ayto-einai-sovaro-provlima/
- Theodorou A, Papaioannou Ch, Roditis K, Tsiapakidou S, Panou Ch, Giorgalla V, Koutsostathis E, Galanakis N, and Vavouranakis Ch. on behalf of JDN-Hellas & Panhellenic Medical Association. Evaluation of the professional development and training of junior doctors in Greece: First results of the “Barometer for junior doctors” [Internet]. Athens: Athens Medical Society. Abstracts Book of the 51st Panhellenic Medical Congress; 24 May 2025 [cited 2025 Oct 14]. Abstract available at: https://www.mednet.gr/sites/default/files/51-EPIS-Abstracts-Book_final.pdf
- Pereira-Neves A, Domingos LF, Ancetti S. The Impact of the First COVID-19 Wave on European Vascular Education. EJVES Vasc Forum. 2022;54:54-57.
- Wippel D. Closing the Gaps in Vascular Training: The EVaST Survey Launches [Internet]. European Society for Vascular Surgery; 24 Jun 2025 [cited 2025 Oct 14]. Available at: https://esvs.org/blog/2025/06/24/closing-the-gaps-in-vascular-training-the-evast-survey-launches/
- Cerame A, Körner M, Launio S, McCourt E, Montvila A, Ribeiro Mourão F, Roditis K, and Sharma S. On behalf of the European Junior Doctors Association. From Tradition to Transition: European Junior Doctors’ Experiences with Work and Their Impact Brussels: European Junior Doctors Association; 2023; Qualitative report; ISBN 978-2-9603376-1-7. Available at: https://www.juniordoctors.eu/sites/default/files/2023-10/Report%20EJD_2023_1.pdf
Table 1. Sociodemographic variables assessed in the study
|
Gender |
||
|
Male |
10 |
40% |
|
Female |
15 |
60% |
|
Age |
||
|
25-30 |
10 |
40% |
|
31-35 |
9 |
36% |
|
36-40 |
5 |
20% |
|
41-50 |
1 |
4% |
|
Part of JD’s journey |
||
|
PGTa |
16 |
64% |
|
ECSb |
9 |
36% |
|
Specialisations |
||
|
1 |
22 |
88% |
|
>1 |
3 |
12% |
|
Total participants |
25 |
100% |
a PGT=post-graduate training, b ECT=early career specialist
Table 2. Overview of key dimensions explored
|
Dimension |
Description |
|
Job satisfaction |
Opinions of JD on the collective’s job satisfaction |
|
Wellbeing |
Impact of work on JD’s wellbeing, emotions and psychosocial sphere |
|
Job resignations |
Opinions on job resignations of JD |
|
Working experiences |
JD’s work-related experiences and their impact (e.g., working conditions, working hours, workload) |
|
Quality of training |
Impact of work on JD’s skills acquisition, supervision by mentors, PGT programs’ quality |
|
Personal lives |
Impact of work on JD’s personal lives |
|
Gender inequalities |
Gender inequalities experienced by JD regarding work, wellbeing, quality of training |
|
Proposals |
EJD’s proposals or recommendations to improve JD professional satisfaction and wellbeing |
|
Specific issues |
Experiences or impacts related to certain contexts (country, postgraduate training programme, early career specialist or specialty) |
{kind=link}
{kind=link}