Physician modified endografts for complex abdominal aortic aneurysms. Are we ready for the next step? A systematic review of the literature

| Available Online: | March, 2026 |
| Page: | 20–28 |
Author for correspondence:
Georgios I. Karaolanis MD, MSc, PhD, FACS
Consultant Vascular and Endovascular Surgery
Swiss Aortic Center, Department of Vascular Surgery
Inselspital, Bern University Hospital, 3010 Bern, Switzerland
E-mail: drgikaraolanis@gmail.com
doi: 10.59037/cwdawc98
eISSN: 2732-7167 / 2026 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Georgios I. Karaolanis1,2, Drosos Kotelis1, Vladimir Makaloski1
1 Swiss Aortic Center Bern, Department of Vascular Surgery, Inselspital, University Hospital of Bern, 3010 Bern, Switzerland
2 Vascular Unit, Department of Surgery, University Hospital of Ioannina and School of Medicine, Ioannina, Greece
Full Text
Gallery
Full Text
Abstract:
Introduction: Physician-modified endografts (PMEGs) have emerged as an alternative endovascular solution for the treatment of complex abdominal aortic aneurysms, particularly when custom-made devices are unavailable or unsuitable due to anatomical constraints or urgent clinical presentation. However, evidence regarding their safety, feasibility, and durability remains heterogeneous.
Methods: A systematic review of the literature was performed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA guidelines). Studies reporting outcomes of PMEGs for complex abdominal aortic aneurysms were identified through a comprehensive search of major medical databases. Early outcomes, including 30-day mortality, aorta-related mortality, technical success, major adverse events (MAEs), and reintervention rates, as well as late outcomes such as overall and aorta-related mortality and reinterventions, were analyzed.
Results: The available literature consisted predominantly of retrospective cohort studies. Technical success rates were high across studies. Early mortality and aorta-related mortality were generally acceptable, although outcomes varied depending on clinical presentation, with a relevant proportion of procedures performed in urgent or emergent settings. MAEs included spinal cord ischemia, myocardial infarction, respiratory failure, stroke, bowel ischemia, and renal failure, not all of which were directly attributable to aortic-related events. Early and late reintervention rates were mainly associated with endoleaks and target vessel complications.
Conclusion: Physician-modified endografts represent a feasible and effective endovascular option for selected patients with complex abdominal aortic aneurysms, particularly in experienced centers and time-sensitive clinical scenarios. While early and mid-term outcomes are encouraging, the current evidence base remains limited by heterogeneity and lack of long-term follow-up. Further prospective studies, standardized reporting, and multicenter registries are required to better define durability, optimize patient selection, and update current guideline recommendations.
Keywords: physician modified endograft, PMEG, complex, abdominal aortic aneurysm, systematic review
INTRODUCTION
The rapid evolution of innovative technologies led to the appropriate development of endovascular techniques for treating complex aortic cases.1,2 Custom-made devices are considered the gold standard of the technological progress, with the companies working hard to make grafts tailored to the patient’s anatomy, allowing for optimal alignment between graft and target vessels, succeeding parallel favourable outcomes regarding aneurysm exclusion and survival.1,3 However, the manufacturing time, cost, and limited availability of custom-made devices restrict their widespread use, particularly in urgent or emergent settings.4 Several solutions to overcome this issue have been proposed, including the off-the-shelf branched stent grafts,5,6 parallel endografts,7,8 and the physician-modified endografts (PMEGs).9-11
Physician-modified endografts have gained increasing popularity since 2010, following the first description by Starnes of modifications or adaptations of commercially available aortic stent grafts replicating fenestrated and branched devices already used in Europe and Asia or available as investigational devices in the United States.12 The rationale behind using these devices is to nullify the patients’ waiting time, creating fenestrations and/or branches for aortic arch, visceral and renal vessels, thereby constituting the most reliable alternative of CMDs.9-11
The aim of the present study was to review the literature and summarize all available data on physician-modified endografts for the treatment of complex aortic diseases involving the aortic arch and the abdominal aorta.
METHODS
Design and registration
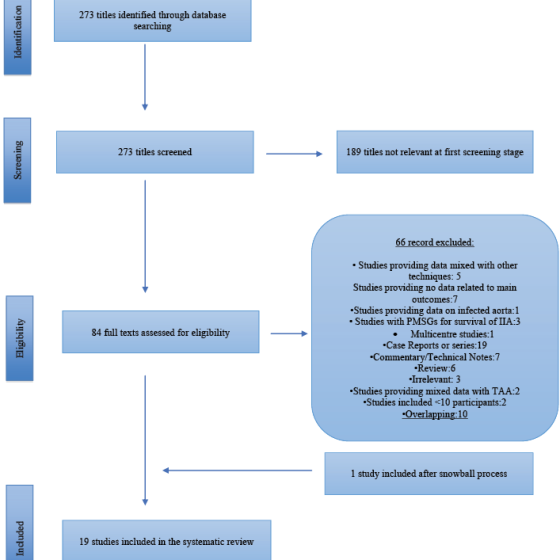
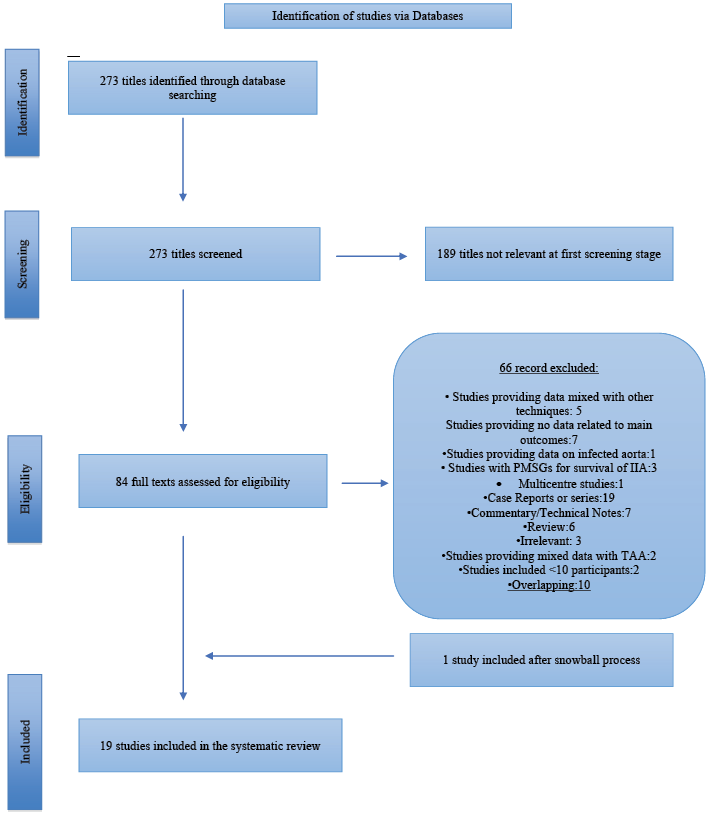
The present systematic review was designed and reported in accordance with the Preferred Reporting Items for Systematic Reviews (PRISMA) statement (Figure 1).
Eligibility criteria
Studies published in English that reported on physician-modified endografts for thoracoabdominal and pararenal aortic aneurysms were included in the present systematic review. At least one target vessel (including renal arteries, coeliac trunk, or mesenteric arteries) had to be included with either a branched (including side branch, inner branch, antegrade, and retrograde) or fenestrated (including reinforced and non-reinforced, and mini cuff reinforced fenestrations) technique for the study to be eligible. Graft modifications that did not include adding a fenestration or branch to the main aortic graft for target vessel revascularisation were excluded. Case reports and case series of 10 patients or less were excluded. The following were also excluded: studies that provided mixed outcomes with other endovascular techniques or had not provided data regarding the main outcomes, review articles, commentary and technical notes, editorials and letters. Multicenter studies that included vascular centers reporting their experiences separately were also excluded to avoid overlap and overestimation of the data.
Search strategy
A thorough literature search was conducted in MEDLINE (via PubMed; 1966 to November 2025), EMBASE (via Ovid; 1980 to November 2025), the Cochrane Central Register of Controlled Trials (CENTRAL) (through November 2025), and Google Scholar (through November 2025). A snowball process of the reference lists from the eligible studies was following the retrieval of relevant reports from the databases searches. The following search items, including expanded Medical Subject Headings (MeSH) terms were used in various combinations: ((physician-modified) OR (surgeon-modified) OR (home-made) OR (back-table)) AND (fenestrated) AND (branched) AND (aorta) AND aneurysm). Figure 1 depicts the eligible studies available in the literature, including 19 retrospective studies.12-30
Definitions
Technical success was defined as satisfactory deployment of the PMEG, successful catheterisation of all fenestration(s)/branches and deployment of the intended bridging stents/stent grafts into the target vessel(s), with patency of the endograft and all target vessels as evidenced by intra-operative completion angiography.2
Fenestration was defined as a constructed hole in the main aortic endograft for catheterization of the visceral vessels and the deployment of the intended bridging stent graft. Branch was defined as a side or inner branch attached to the main endograft prior to its deployment.2
Major adverse events at 30-days were defined as all-cause mortality, myocardial infarction, respiratory failure requiring prolonged (>24 hours from anticipated) mechanical ventilation or reintubation, renal function decline resulting in >50% reduction in baseline eGFR or new-onset dialysis, bowel ischemia requiring surgical resection or not resolving with medical therapy, major stroke, and paraplegia.2
Preoperative planning and Technique
Preoperative planning for physician-modified endografts is routinely based on high-resolution computed tomography angiography with thin-slice acquisition (<1mm) and advanced multiplanar and three-dimensional reconstruction. This imaging approach allows accurate assessment of vascular anatomy, including the identification of target vessel origin, diameter, and the inter-vessel distances required for appropriate fenestration planning.31
The technique for mapping fenestration location differs among operators.24,32 The use of three-dimensional printed templates to assist with fenestration alignment has been explored, particularly among less experienced operators.24 Available evidence indicates that these adjunctive tools may enhance the precision of fenestration transfer when resources allow; however, clinical outcomes remain closely linked to institutional expertise in complex aortic repair.24,32 Recently, a new software has been proposed for more precise design and construction of fenestrations.15 The punch card technique was developed to eliminate the 3D printing workflow while preserving the benefits of having a 3D model.32
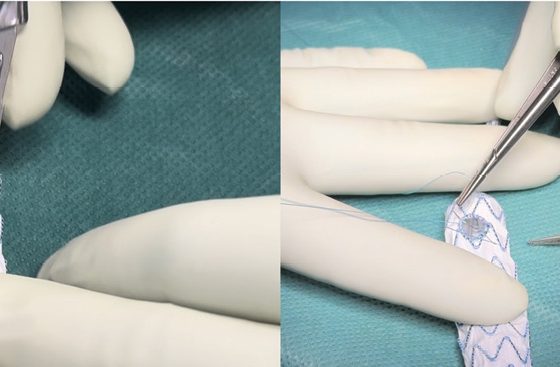
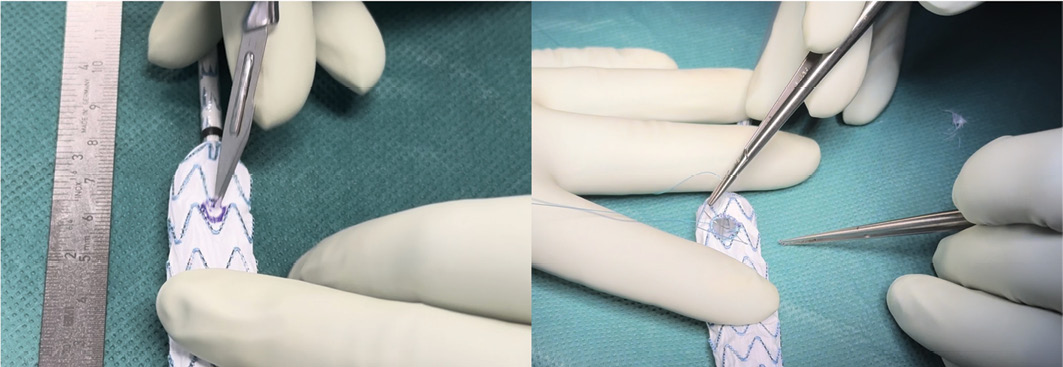
The physician-modification technique has been previously described in detail.33 After partial deployment of the first stent graft rings on a back table, proximal markers are used to orientate on the endograft, and a curved clamp is utilized to unfold the fabric for placement of the fenestrations. (Figure 2) The position of the fenestrations was marked with a sterile pen through the holes of the punch card, and the preparation was continued in a standard fashion. Considerable technical heterogeneity was observed with respect to the instruments used for fenestration creation. While some operators favor the use of a scalpel, others prefer ophthalmic cautery.33-35 This divergence is largely driven by concerns that the use of ophthalmic cautery may weaken the graft fabric compared with mechanical cutting using a scalpel; however, this hypothesis has not yet been definitively proven. The created fenestrations were reinforced using a double-layer Goose Snare wire (ev3 Endovascular, Plymouth, MN, USA) or alternative materials, such as loops cut from snares or the tip of a radiopaque wire, and secured with a running 4-0 polyfilament suture.33, 35 Re-sheathing of the PMEG was performed using vessel loops or Mersilene bands.33, 35
In published reports, incorporation of target vessels in physician-modified endografts has most commonly been accomplished using fenestrations, although the use of scallops and directional branches has also been described.25,28,36,37 (Table 1) Several studies have highlighted anatomical factors that may guide the selection of the incorporation strategy. Fenestrations are generally favored for target vessels with upward or transverse orientations and in cases involving relatively narrow aortic diameters, whereas directional branches are more frequently applied to caudally oriented vessels or those originating from widened aortic segments.16, 38 Despite these proposed considerations, no consensus has emerged regarding the optimal choice among fenestrations, scallops, and branches, and marked variability in technique persists across reported series.25, 28, 36, 37
Type of modified endografts
Endografts manufactured from Dacron or polytetrafluoroethylene (PTFE) were the most frequently reported devices across the available literature. Commonly used platforms included the Zenith TX2 and Zenith Alpha systems (Cook Medical, Bloomington, IN), the TREO stent graft (Terumo Aortic, Tokyo, Japan), as well as the Valiant Captivia and Endurant devices (Medtronic, Minneapolis, MN).16,28,33,36 At present, there is no clear evidence regarding the optimal endograft material for the construction of physician-modified endografts. A recent small retrospective cohort study evaluated the use of polytetrafluoroethylene endografts for physician-modified endografts.39 Over a short follow-up period of seven months, the authors reported one case of type Ic endoleak and six cases of type II endoleaks, with a reintervention rate of 12%.39 While most published studies have focused on Dacron-based grafts for physician-modified endografts, this report explored the use of polytetrafluoroethylene-based devices, citing improved ease of manipulation and implantation. Nevertheless, further evidence is required to validate these findings.
RESULTS
Physician modified endografts for reno-visceral segments
A total of 19 retrospective studies published between 2012 and 2025 were included in this systematic review. Of the 1595 (mean age 73 (67-79) years) patients included, 1252 (78%) were male. Of them, 93% (1478 of 1595) had hypertension, 48% (759 of 1595) had coronary artery disease, 49% (788 of 1595) dyslipidaemia, 27% (427 of 1595) chronic kidney disease, 9% (136/1595) history of cerebrovascular diseases, 40% (606/1595) chronic obstructive pulmonary disease and 19% diabetes (311 of 1595), 32% (507/1595) had prior aortic procedure whereas 45% (717/1595) were active smokers.
Operative Details
Of the procedures, 62% had been elective, 24% had been emergent and 15% urgent. Physician-modified endografts were almost equally used for PRAA (56%) and TAAA (44%). Overall, 4204 target vessels were addressed through fenestrations, branches, or scallop configuration. Ten out of the nineteen studies reported on fenestration (n=3961)12, 13, 15, 17, 18, 21, 24, 25, 27, 28 while the rest reported on combined branched and fenestrated (n=243) repair.14, 16, 20, 22-24, 26, 29, 30
The mean operative time ranged from 138 to 453 minutes (reported in 17 studies),12-30 the mean fluoroscopy time from 39 to 136 minutes (reported in 15 studies),12, 14-23, 25-30 the contrast medium from 70 to 235 mL (reported in 16 studies)12, 14-30 and the estimated blood loss from 120 to 936 ml (reported in eight studies).12, 16, 17, 19, 23, 26, 28, 30 The mean length of stay was reported in 15 studies, 12, 19, 20, 23, 27-39 ranging from 4 to 17 days and the intensive care unit stay ranged from 2 to 4 days (reported in six studies). The mean follow-up was reported in all included studies, varied between 1 to 47 months.12-30 (Table 1)
Early outcomes
The technical success of PMEGs ranged from 87% to 100% among the studies.12-30 (Table 2) Chan et al.17 reported the lower technical success rate of 87%. Recently, our group reported that the pooled technical success in elective cases was 98.6% (95% CI 97.2-99.3%, p<0.001, I^2=83%;), while in the emergent/urgent group, it was 95.1% (95% CI 90.5-97.5%, p<0.15, I^2=39%;).10
The 30-day mortality among the studies ranged from 0% to 18.9%.12-30 Scali et al.26 reported the highest crude 30-day mortality rate of 18.9% (7/37 patients) (Table 2). It is worth mentioning that this study reported outcomes in emergent and/or urgent settings. The aorta related mortality ranged from 0.3% to 9.5%.12-30 Tsilimparis et al29 reported the highest aorta related mortality rate of 9.5%.
The early major adverse events rate among the studies ranged from 1.8% to 50%.12-30 Ricotta et al.23 reported the highest MAE rate of 50% (6/12 patients) (Table 2). A more detailed analysis of major adverse events showed rates of spinal cord ischemia ranging from 2% to 7.6%,14, 16-19, 21, 22, 24-27, 29, 30 myocardial infarction from 3.5% to 4%,14, 16-19, 21, 22, 24-27, 29, 30 respiratory failure from 5% to 7.5%,14, 16-19, 21, 22, 24-27, 29, 30 stroke from 2% to 3.5%, 14, 16-19, 21, 22, 24-27, 29, 30 bowel ischemia from 1.1% to 5.8%,14, 16-19, 21, 22, 24-27, 29, 30 and new-onset hemodialysis from 2.2% to 3.4%.14, 16-19, 21, 22, 24-27, 29, 30
The early reintervention rate ranged from 0% to 31% 12, 13, 15-17, 19-27, 29, 30 The most common aetiology was type II endoleak followed by Ia, Ic and IIIc.2, 12, 13, 15, 17, 19, 21, 26, 27, 29 Our group reported that the pooled rate of target vessel instability was 1.9% (95% CI 1.1-3.2%, p=0.00, I^2=80%;).10
Late outcomes
At a mean of 18 (1-47) months of follow-up (Table 1), late mortality among the studies ranged from 0% to 39%.12, 13, 15-17, 19, 21, 23, 24, 26, 28-30 Rynio et al24 reported the highest crude 30-day mortality rate of 39%, however, this percentage is not strictly related with aorta-specific events. (Table 2)
The late aorta related mortality ranged from 1.0% to 9.5%.12, 13, 15-17, 19, 21, 23, 24, 26, 28-30 Tsilimparis et al29 reported the highest crude 30-day aorta related mortality rate of 9.5%. It should be noted that this study reported outcomes exclusively in emergent or urgent settings. (Table 2)
The late major adverse events rate among the studies ranged from 2.1% to 28%.12,13,25,27 Sénémaud et al27 reported the highest rate of 28% (8/28 patients) (Table 2). In this study spinal cord injury was observed in 7% (2/28) patients, while transient renal failure was detected in 14% (4/28) patients.
The late reintervention rate ranged from 0% to 37% among the studies.12-24, 26, 29, 30 Chait et al.16 reported the highest reintervention rate of 37% (57/156 patients). Of them, 33 were due to endoleak of bridging stents grafts, 20 for bridging stents stenosis and the rest (n=16) due to access related complications.
Discussion
This systematic review summarizes the available evidence on physician-modified endografts for the treatment of complex aortic diseases, with particular emphasis on early and late clinical outcomes. Overall, the findings suggest that physician-modified endografts represent a feasible and effective treatment option in selected patients, achieving acceptable rates of technical success, early mortality, and mid-term outcomes, particularly in settings where custom-made devices are unavailable or unsuitable.
Early outcomes demonstrated high technical success rates across the included studies, reflecting the growing expertise of specialized centers in planning, device modification, and implantation techniques.34, 36 Thirty-day mortality and aorta-related mortality were generally low and comparable to those reported for alternative endovascular strategies in complex aortic repair.6 However, it is important to note that a substantial proportion of the reported experience involved urgent or emergent cases, which may partly explain the observed variability in early mortality and major adverse event rates.6, 26, 29, 30
Major adverse events remained a relevant concern, with reported complications including spinal cord ischemia, myocardial infarction, respiratory failure, stroke, bowel ischemia, and new-onset renal failure requiring hemodialysis.14, 16-19, 21, 22, 24-27, 29, 30 Importantly, not all major adverse events were directly attributable to aortic-related causes, highlighting the complexity of the treated population and the significant burden of comorbidities. These findings underscore the need for careful patient selection, meticulous perioperative management, and the implementation of established protective strategies, particularly in extensive thoracoabdominal repairs.10, 36
Reintervention rates in the early postoperative period were acceptable and most commonly related to endoleaks or target vessel issues. Type II endoleaks were frequently reported but were often managed conservatively, whereas type I and type III endoleaks more frequently required secondary interventions.2,12,13,15,17,19, 21, 26, 27, 29 These observations reinforce the importance of accurate fenestration or branch alignment and durable target vessel incorporation. Limited data are available in the literature regarding the type of bridging stent grafts used, therefore, it remains difficult to draw firm conclusions, about which BSG is optimal.10 Comparing these rates with other endovascular techniques seem identical.40 Two multicenter studies34,36 based on PMEGs showed a freedom of reintervention of 73.8%, 61.8%, and 51.4% at 1, 3, and 5 years respectively, which is consistent with the results reported on CMDs.40-42
With regard to late outcomes, overall survival and aorta-related survival appeared favorable in the available mid-term follow-up, although long-term data remain limited.12, 13, 15-17, 19, 21, 23, 24, 26, 28-30 Late reinterventions were reported in a subset of patients and were primarily related to endoleaks, bringing stents instability, or disease progression. Our group, reported a pooled late bridging stent instability rate of 13.9%.10 In the elective group, the late reintervention rate was 14.6% (95% CI 7.5%-26.5%, p=0.00, I2=43%) while for the emergent/urgent group, it was 15.6%. Another factor that appears to have influenced the survival related outcomes seems to be the high American Society of Anesthesiologists (ASA) score and the low estimated glomerular filtration rate observed in these patients.36 As a result, outcomes were worse than expected, suggesting that these variables may be useful in improving patient selection. The need for secondary procedures highlights the importance of structured imaging surveillance following physician-modified endograft implantation, particularly given the customized nature of these devices.
Considerable heterogeneity was observed across studies in terms of device platforms, modification techniques, fenestration design, and materials used for reinforcement.12, 13, 15, 17, 18, 21, 24, 25, 27, 28,32-38 While most reports favored Dacron-based endografts, emerging data on polytetrafluoroethylene-based devices suggest potential advantages in handling and implantation; however, current evidence is insufficient to define an optimal endograft material.39 Similarly, no consensus has been reached regarding the optimal strategy for target vessel incorporation, with fenestrations, scallops, and directional branches each being applied according to anatomical considerations and operator preference.
In the 2024 ESVS abdominal aorto-iliac aneurysm guidelines, PMEGs (and in situ laser fenestration) are specifically recommended to be reserved for urgent patients when the manufacturing delay for a custom-made device is too long or when no suitable off-the-shelf option exists, and urgent/ruptured complex AAA repair may be considered using these strategies based on patient status, anatomy, and preferences (Class IIa, Level C).1
This systematic review has several limitations. First, all included studies were retrospective observational cohorts, which may introduce selection bias and limit the generalizability of the findings. Second, considerable heterogeneity existed among studies regarding patient selection, device platforms, modification techniques, and outcome reporting. Third, due to variability in outcome definitions and reporting across studies, a formal quantitative meta-analysis could not be reliably performed. Finally, long-term follow-up data remain limited, highlighting the need for prospective studies and multicenter registries to better define the durability and safety of physician-modified endografts.
CONCLUSION
Physician-modified endografts appear to be a valuable endovascular option for the management of complex aortic diseases, demonstrating acceptable early and late outcomes when performed in experienced centers. While current evidence supports their use in selected clinical scenarios, particularly in urgent or emergent settings, further prospective studies and standardized reporting are needed to better define long-term durability, optimal device selection, and patient-specific indications.
REFERENCES
- Wanhainen A, Van Herzeele I, Bastos Goncalves F, Bellmunt Montoya S, Berard X, Boyle JR, et al. Editor’s Choice — European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. Eur J Vasc Endovasc Surg. 2024;67(2):192-331.
- Oderich GS, Forbes TL, Chaer R, Davies MG, Lindsay TF, Mastracci T, et al. Reporting standards for endovascular aortic repair of aneurysms involving the renal-mesenteric arteries. J Vasc Surg. 2021;73(1S):4S-52S.
- Wanhainen A, Gombert A, Antoniou GA, Fidalgo Domingos LA, Gouveia EMR, Grabenwoger M, et al. European Society for Vascular Surgery (ESVS) 2026 Clinical Practice Guidelines on the Management of Descending Thoracic and Thoraco-Abdominal Aortic Diseases. Eur J Vasc Endovasc Surg. 2025.
- Gallitto E, Faggioli G, Spath P, Pini R, Mascoli C, Ancetti S, et al. The risk of aneurysm rupture and target visceral vessel occlusion during the lead period of custom-made fenestrated/branched endograft. J Vasc Surg. 2020;72(1):16-24.
- Farber MA, Oderich GS, Timaran C, Sanchez LA, Dawson Z, Zenith p-Branch Feasibility Study I. Results from a prospective multicenter feasibility study of Zenith p-Branch stent graft. J Vasc Surg. 2019;70(5):1409-18 e3.
- Karaolanis GI, Makaloski V, Jungi S, Weiss S, Kotopoulos K, Chaikhouni B, et al. Endovascular repair of pararenal and thoracoabdominal aortic aneurysms with inner and outer off-the-shelf multibranched endografts: A systematic review and meta-analysis. J Vasc Surg. 2025;81(1):251-60.e3.
- Donas KP, Torsello GB, Piccoli G, Pitoulias GA, Torsello GF, Bisdas T, et al. The PROTAGORAS study to evaluate the performance of the Endurant stent graft for patients with pararenal pathologic processes treated by the chimney/snorkel endovascular technique. J Vasc Surg. 2016;63(1):1-7.
- Karaolanis GI, Pipitone MD, Torsello G, Austermann M, Donas KP. Endovascular treatment of proximal para-anastomotic aneurysms after previous surgical repair of infrarenal aortic aneurysms by the chimney technique. Vascular. 2019;27(1):3-7.
- Karaolanis GI, Papazoglou DD, Donas KP, Helfenstein F, Kotelis D, Makaloski V. Physician-modified versus chimney endografting for pararenal aortic aneurysms: a systematic review and meta-analysis. J Cardiovasc Surg (Torino). 2024;65(2):124-31.
- Karaolanis GI, Kotopoulos K, Dabravolskaite V, Peroulis MG, Bosiers MJ, Kotelis D, et al. High Technical Success and Low Reintervention Rate of Physician-Modified Endografts for Reno-Visceral Aortic Pathologies: Systematic Review and Meta-Analysis. J Endovasc Ther. 2025:15266028251388732.
- Karaolanis GI, Makaloski V, Jungi S, Celik M, Bosiers MJ, Kotelis D. Endovascular Repair of Aortic Arch Zones 0 to 2 Using Physician-Modified Endografts: A Systematic Review and Meta-Analysis. J Endovasc Ther. 2024:15266028241292485.
- Starnes BW. Physician-modified endovascular grafts for the treatment of elective, symptomatic, or ruptured juxtarenal aortic aneurysms. J Vasc Surg. 2012;56(3):601-7.
- Alvarez Marcos F, Reyes Valdivia A, De Blas Bravo M, Alonso Perez M. Physician-Modified Endografts for Non-deferrable Complex Abdominal Aortic Aneurysm Repair Using the Endurant Platform: Templates and Initial Results. J Endovasc Ther. 2025:15266028251318952.
- Asirwatham M, Konanki V, Lucas SJ, Grundy S, Zwiebel B, Shames M, et al. Comparative outcomes of physician-modified fenestrated/branched endovascular aortic aneurysm repair in the setting of prior failed endovascular aneurysm repair. J Vasc Surg. 2023;78(5):1153-61.
- Branzan D, Geisler A, Grunert R, Steiner S, Bausback Y, Gockel I, et al. The Influence of 3D Printed Aortic Models on the Evolution of Physician Modified Stent Grafts for the Urgent Treatment of Thoraco-abdominal and Pararenal Aortic Pathologies. Eur J Vasc Endovasc Surg. 2021;61(3):407-12.
- Chait J, Tenorio ER, Hofer JM, DeMartino RR, Oderich GS, Mendes BC. Five-year outcomes of physician-modified endografts for repair of complex abdominal and thoracoabdominal aortic aneurysms. J Vasc Surg. 2023;77(2):374-85 e4.
- Chan HL, Papazoglou DD, Jungi S, Weiss S, Becker D, Kotelis D, et al. Fenestrated Physician-Modified Endografts for Preservation of Main and Accessory Renal Arteries in Juxtarenal Aortic Aneurysms. J Clin Med. 2023;12(14).
- Dossabhoy SS, Simons JP, Flahive JM, Aiello FA, Sheth P, Arous EJ, et al. Fenestrated endovascular aortic aneurysm repair using physician-modified endovascular grafts versus company-manufactured devices. J Vasc Surg. 2018;67(6):1673-83.
- Han JY, DiBartolomeo AD, Pyun AJ, Hong YH, Paige JF, Magee GA, et al. Impact of Combining Iliac Branch Endoprosthesis and Physician-Modified Fenestrated-Branched Endovascular Repair for Complex Abdominal and Thoracoabdominal Aortic Aneurysms with Concomitant Iliac Artery Aneurysms. Ann Vasc Surg. 2025;111:13-24.
- Juszczak MT, Vezzosi M, Khan M, Mascaro J, Claridge M, Adam D. Endovascular repair of acute juxtarenal and thoracoabdominal aortic aneurysms with surgeon-modified fenestrated endografts. J Vasc Surg. 2020;72(2):435-44.
- Nguyen T, Gittinger M, Gryzbowski C, Patel S, Asirwatham M, Grundy S, et al. One-hundred Consecutive Physician-Modified Fenestrated Endovascular Aneurysm Repair of Pararenal and Thoracoabdominal Aortic Aneurysms Using the Terumo TREO Stent Graft. Ann Vasc Surg. 2024;106:369-76.
- Oderich GS, Ribeiro MS, Sandri GA, Tenorio ER, Hofer JM, Mendes BC, et al. Evolution from physician-modified to company-manufactured fenestrated-branched endografts to treat pararenal and thoracoabdominal aortic aneurysms. J Vasc Surg. 2019;70(1):31-42 e7.
- Ricotta JJ, 2nd, Tsilimparis N. Surgeon-modified fenestrated-branched stent grafts to treat emergently ruptured and symptomatic complex aortic aneurysms in high-risk patients. J Vasc Surg. 2012;56(6):1535-42.
- Rynio P, Jedrzejczak T, Rybicka A, Milner R, Gutowski P, Kazimierczak A. Initial Experience with Fenestrated Physician-Modified Stent Grafts Using 3D Aortic Templates. J Clin Med. 2022;11(8).
- Sanders AP, Gomez-Mayorga J, Manchella MK, Swerdlow NJ, Schermerhorn ML. Ten years of physician-modified endografts. J Vasc Surg. 2025;81(1):1-12 e1.
- Scali ST, Neal D, Sollanek V, Martin T, Sablik J, Huber TS, et al. Outcomes of surgeon-modified fenestrated-branched endograft repair for acute aortic pathology. J Vasc Surg. 2015;62(5):1148-59 e2.
- Senemaud JN, Ben Abdallah I, de Boissieu P, Touma J, Kobeiter H, Desgranges P, et al. Intraoperative adverse events and early outcomes of custom-made fenestrated stent grafts and physician-modified stent grafts for complex aortic aneurysms. J Vasc Surg. 2020;71(6):1834-42 e1.
- Starnes BW, Zettervall S, Larimore A, Singh N. Long-Term Results of Physician-Modified Endografts for the Treatment of Elective, Symptomatic, and Ruptured Juxtarenal Abdominal Aortic Aneurysms. Ann Surg. 2024;280(4):633-9.
- Tsilimparis N, Heidemann F, Rohlffs F, Diener H, Wipper S, Debus ES, et al. Outcome of Surgeon-Modified Fenestrated/Branched Stent-Grafts for Symptomatic Complex Aortic Pathologies or Contained Rupture. J Endovasc Ther. 2017;24(6):825-32.
- Yang G, Zhang Y, Ni H, Zhang L, Wang P, Li X, et al. Result of a Multicenter Study on the Physician-Modified Fenestrated and Branched Endovascular Grafts for Thoracoabdominal Aneurysms. Ann Thorac Surg. 2025;119(6):1241-8.
- Canonge J, Jayet J, Heim F, Chakfe N, Coggia M, Coscas R, et al. Comprehensive Review of Physician Modified Aortic Stent Grafts: Technical and Clinical Outcomes. Eur J Vasc Endovasc Surg. 2021;61(4):560-9.
- Juhos B, Szentivanyi A, Berczi A, Huttl A, Borzsak S, Szablics F, et al. A Novel Surgical Software Tool to Improve the Physician-Modified Endograft Workflow. J Endovasc Ther. 2026:15266028251406185.
- Papazoglou DD, Karaolanis GI, Kotelis D, Makaloski V. Physician-Modified Endografts with the TREO Stent Graft System. J Endovasc Ther. 2024:15266028241282643.
- Csobay-Novak C, Dionisi CP, Szentivanyi A, Berczi A, Osztrogonacz P, Di Sabato A, et al. Physician-Modified Endografts in Elective Care: A Report From the REgistry of MOdified Treo Endografts in Europe (REMOTE). J Endovasc Ther. 2026:15266028251405754.
- Stana J, Bertrand L, Assaf B, Khangholi DB, Konstantionou N, Tsilimparis N. Optimizing PMEG Technique: Enhancing Endovascular Repair With Pre-Manufactured Fenestrated Endografts. J Endovasc Ther. 2025:15266028251397850.
- Tsilimparis N, Gouveia EMR, Tenorio ER, Scali S, Mendes B, Han S, et al. Multicenter Study on Physician-Modified Endografts for Thoracoabdominal and Complex Abdominal Aortic Aneurysm Repair. Circulation. 2024;150(17):1327-42.
- Smith JA, Sarode AL, Stern JR, Cho JS, Harth K, Wong V, et al. Physician-modified endografts are associated with a survival benefit over parallel grafting in thoracoabdominal aneurysms. J Vasc Surg. 2022;76(2):318-25 e4.
- Torrealba J, Panuccio G, Kolbel T, Gandet T, Heidemann F, Rohlffs F. Physician-Modified Endograft With Inner Branches for the Treatment of Complex Aortic Urgencies. J Endovasc Ther. 2022;29(5):697-704.
- Zambetti BR, Shiva A, Hardy JT, Babick OM, DeMartino AG, Shah NN, et al. Physician Modification of Polytetrafluoroethylene Based Endografts for Aortic Aneurysm Repair. J Endovasc Ther. 2025:15266028251353359.
- Patel SR, Ormesher DC, Griffin R, Jackson RJ, Lip GYH, Vallabhaneni SR, et al. Editor’s Choice – Comparison of Open, Standard, and Complex Endovascular Aortic Repair Treatments for Juxtarenal/Short Neck Aneurysms: A Systematic Review and Network Meta-Analysis. Eur J Vasc Endovasc Surg. 2022;63(5):696-706.
- Roy IN, Millen AM, Jones SM, Vallabhaneni SR, Scurr JRH, McWilliams RG, et al. Long-term follow-up of fenestrated endovascular repair for juxtarenal aortic aneurysm. Br J Surg. 2017;104(8):1020-7.
- Tenorio ER, Mirza AK, Lima GBB, Marcondes GB, Wong J, Mendes BC, et al. Characterization of Secondary Interventions After Fenestrated-branched Endovascular Repair of Complex Aortic Aneurysms and Its Effect on Quality of Life and Patient Survival. Ann Surg. 2023;278(1):140-7.
Table 1: Baseline characteristics of PMEGs studies for reno-visceral segment
|
Investigator |
Year |
Participants No |
Type of Presentation |
Aortic Diameter (mm) |
Morphology of PMEGs (n) |
Mean follow-up period (months) |
||||
|
Elective |
Urgent |
Emergent |
Fenestrations |
Branches |
Scallop |
|||||
|
Yang et al32 |
2025 |
186 |
104 |
82 |
nr |
56 |
530 |
86 |
2 |
40 |
|
Alvarez et al26 |
2025 |
18 |
12 |
nr |
6 |
70 |
37 |
nr |
nr |
10 |
|
Sanders et al20 |
2024 |
184 |
165 |
18 |
1 |
62 |
691 |
nr |
nr |
nr |
|
Han et al39 |
2025 |
161 |
111 |
2 |
48 |
68 |
nr |
nr |
nr |
23 |
|
Starnes et. al19 |
2024 |
203 |
NR |
NR |
NR |
67 |
237 |
nr |
nr |
12 |
|
Nguyen et al27 |
2024 |
100 |
94 |
4 |
2 |
66 |
383 |
nr |
nr |
10 |
|
Asirwatham et al33 |
2023 |
103 |
91 |
8 |
4 |
66 |
383 |
7 |
nr |
7 |
|
Chan et. Al28 |
2023 |
37 |
34 |
2 |
1 |
64 |
37 |
nr |
nr |
18 |
|
Chait et. Al23 |
2022 |
156 |
128 |
16 |
12 |
70 |
407 |
16 |
29 |
47 |
|
Rynio et al14 |
2022 |
43 |
34 |
nr |
9 |
62 |
162 |
nr |
nr |
14 |
|
Branzan et al29 |
2021 |
19 |
nr |
6 |
13 |
72 |
71 |
nr |
nr |
14 |
|
Sénémaud Jn et al30 |
2020 |
28 |
15 |
nr |
13 |
74 |
98 |
nr |
nr |
1 |
|
Juszczak et al34 |
2020 |
54 |
4 |
10 |
40 |
76 |
171 |
nr |
3 |
20 |
|
Oderich et al35 |
2019 |
145 |
145 |
nr |
nr |
69 |
393 |
21 |
39 |
38 |
|
Dossabhoy et al31 |
2018 |
41 |
32 |
9 |
nr |
65 |
106 |
nr |
nr |
21 |
|
Tsilimparis et al21 |
2017 |
21 |
nr |
13 |
8 |
74 |
58 |
2 |
9 |
13 |
|
Scali et al37 |
2015 |
37 |
nr |
10 |
27 |
73 |
82 |
23 |
4 |
8 |
|
Starnes et. Al19 |
2012 |
47 |
9 |
nr |
38 |
61 |
82 |
nr |
nr |
20 |
|
Ricotta JJ et al38 |
2012 |
12 |
nr |
5 |
7 |
81 |
33 |
2 |
nr |
9 |
|
Overall |
2012-2025 |
1595 |
978 |
185 |
229 |
56-81 |
3961 |
157 |
86 |
18 (1-47) |
Table 2: Early outcomes of PMEGs studies
|
Investigator |
Technical success per patient (%) |
30-day Aorta related mortality(n) |
30-day Mortality (n) |
Early MAE (n) |
Early Reintervention (n) |
Patency Rate of visceral grafts (n) |
|
Yang et al32 |
98% |
2 |
6 |
34 |
10 |
614/618 |
|
Alvarez et al26 |
100% |
nr |
0 |
nr |
0 |
36/37 |
|
Sanders et al20 |
100% |
0 |
9 |
53 |
58 |
691 |
|
Han et al39 |
92% |
5 |
8 |
36 |
8 |
574/576 |
|
Starnes et. Al19 |
94% |
0 |
6 |
29 |
nr |
540/575 |
|
Nguyen et al27 |
99% |
1 |
2 |
25 |
2 |
382/383 |
|
Asirwatham et al33 |
99% |
nr |
3 |
22 |
nr |
nr |
|
Chan et. Al28 |
87% |
0 |
0 |
5 |
2 |
41/47 |
|
Chait et. Al23 |
99% |
2 |
9 |
40 |
0 |
NR |
|
Rynio et al14 |
86% |
0 |
5 |
5 |
2 |
162/162 |
|
Branzan et al29 |
100% |
0 |
0 |
4 |
2 |
70/71 |
|
Sénémaud Jn et al30 |
100% |
1 |
4 |
4 |
9 |
98/98 |
|
Juszczak et al34 |
100% |
nr |
9 |
1 |
3 |
182/189 |
|
Oderich et al35 |
98% |
NR |
8 |
70 |
18 |
438/447 |
|
Dossabhoy et al31 |
nr |
nr |
2 |
18 |
nr |
106 |
|
Tsilimparis et al21 |
100% |
2 |
3 |
6 |
2 |
69/69 |
|
Scali et al37 |
92% |
nr |
7 |
15 |
5 |
96/105 |
|
Starnes et. Al19 |
98% |
0 |
1 |
3 |
3 |
80/82 |
|
Ricotta JJ et al38 |
100% |
0 |
1 |
6 |
2 |
35/36 |
n: number of cases; nr: no reported; MAE: major adverse events
Table 2 (continue)
Table 2: Late outcomes of PMEGs studies
|
Investigator |
Late Aorta related mortality (n) |
Late Mortality (n) |
Late MAE (n) |
Late Reintervention (n) |
Late Patency Rate of visceral grafts (n) |
|
Yang et al32 |
1 |
2 |
nr |
13 |
209/211 |
|
Alvarez et al26 |
0 |
3 |
0 |
0 |
36/37 |
|
Sanders et al20 |
nr |
nr |
8 |
nr |
nr |
|
Han et al39 |
nr |
44 |
nr |
7 |
nr |
|
Starnes et. Al19 |
3 |
3 |
nr |
nr |
nr |
|
Nguyen et al27 |
0 |
2 |
nr |
7 |
380/383 |
|
Asirwatham et al33 |
nr |
nr |
nr |
10 |
nr |
|
Chan et. Al28 |
0 |
4 |
nr |
8 |
45/47 |
|
Chait et. Al23 |
3 |
3 |
nr |
88 |
nr |
|
Rynio et al14 |
7 |
17 |
nr |
6 |
150/162 |
|
Branzan et al29 |
0 |
1 |
nr |
2 |
69/71 |
|
Sénémaud Jn et al30 |
nr |
nr |
8 |
5 |
98/98 |
|
Juszczak et al34 |
nr |
nr |
nr |
12 |
nr |
|
Oderich et al35 |
0 |
nr |
nr |
42 |
nr |
|
Dossabhoy et al31 |
nr |
nr |
nr |
19 |
nr |
|
Tsilimparis et al21 |
1 |
4 |
nr |
1 |
69/69 |
|
Scali et al37 |
nr |
5 |
nr |
6 |
102/105 |
|
Starnes et. Al19 |
0 |
2 |
1 |
2 |
81/82 |
|
Ricotta JJ et al38 |
1 |
2 |
nr |
0 |
35/36 |
n: number of cases; nr: no reported; MAE: major adverse events
{kind=link}
{kind=link}