Cancer Incidence and Mortality Following EVAR and Open Aneurysm Repair: A Systematic Review

| Available Online: | March, 2026 |
| Page: | 29–36 |
Author for correspondence:
Pavlos Georgiou
1st Department of Vascular Surgery, Attikon University Hospital, National and Kapodistrian University of Athens, Athens, Greece
E-mail: georgioupavlos1604@gmail.com
doi: 10.59037/qbep8r76
eISSN: 2732-7167 / 2026 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
1st Department of Vascular Surgery, Attikon University Hospital, National and Kapodistrian University of Athens, Athens, Greece
Full Text
Gallery
Full Text
Abstract:
Introduction: There is limited evidence in the literature regarding the incidence and mortality of cancer following either open surgical repair (OR) or endovascular aneurysm repair (EVAR) of abdominal aortic aneurysms (AAA). This study aims to compare cancer-related incidence and mortality between EVAR and OR in patients with no pre-existing malignancy.
Methods: Relevant studies were identified through electronic database searches and manual reference screening. The MEDLINE database (via PubMed) was searched using unrestricted strategies combining Medical Subject Headings (MeSH) and keywords. Studies published between 2010 and 2025 were included.
Results: From 710 initial articles, six met the inclusion criteria. These comprised a total of 67,866 patients (85% male), with a mean age of 72.9 ± 1.5 years. There was no significant age difference between EVAR and OR groups (p = 0.42). Among the included population, 48.4% (n=32,880) underwent EVAR, while 51.6% (n=34,986) underwent OR. The average follow-up period across studies was 10.6 years (range 1.8–15.8 years).
Conclusion: Although some studies have reported possible differences in cancer incidence between EVAR and open repair, the findings remain inconsistent and may be affected by variations in patient risk profiles, follow-up protocols, or study design. Future large, methodologically robust studies with standardized data collection and long-term surveillance are needed to clarify whether a true causal relationship exists between EVAR, radiation exposure, and cancer development.
Keywords: abdominal aortic aneurysm, endovascular repair, open repair, malignancy, neoplasm, cancer incidence, cancer mortality
*Introduction
There is limited evidence in the surgical literature regarding the incidence and mortality of cancer following either open surgical repair (OR) or endovascular aortic aneurysm repair (EVAR). Many published studies have primarily focused on patients presenting with both malignancy and abdominal aortic aneurysm (AAA), rather than on the de novo risk of cancer following these procedures.1,2
Over the past two decades, endovascular repair has progressively gained predominance over open surgery in the management of abdominal aortic aneurysms.3 EVAR offers significant perioperative advantages, including reduced morbidity and mortality, shorter hospital stays, and faster recovery.4–6 These benefits have led to its widespread adoption, particularly among elderly or comorbid patients, while open repair is now mainly reserved for anatomically unsuitable cases or younger, low-risk individuals.3
Nevertheless, there is emerging evidence suggesting that the endovascular approach may be associated with a higher long-term risk of developing metachronous malignancies.7–10 This has been attributed to cumulative radiation exposure, both during fluoroscopy-guided procedures and during postoperative CT surveillance, which remains the gold standard for detecting endograft-related complications.11,12 Despite proposed low-dose CT protocols for follow-up, such strategies are not yet routinely implemented in clinical practice.12,13 Notably, in the EVAR-1 trial, an increased rate of aneurysm-related deaths was accompanied by a higher incidence of cancer-related mortality in the EVAR group.4 Similar findings were observed in the EVAR-1, OVER, and DREAM trials, which together reported 2,484 patients with long-term follow-up, confirming that deaths due to aneurysm rupture or cancer were present in both treatment groups. 4,5,6 Interestingly, in the OVER trial, cancer-related mortality was higher in the open repair group than in the endovascular group.5
The aim of this study was to compare cancer-related incidence and mortality between EVAR and OR in patients with no pre-existing malignancy.
METHODS
Search Strategy
Relevant studies were identified through a comprehensive search of electronic databases and a manual review of reference lists. The National Library of Medicine’s MEDLINE database was accessed via the PubMed interface and searched from 1976 to the present.
An unrestricted search strategy was applied using exploded Medical Subject Headings (MeSH) terms and keywords combined with the Boolean operators AND, OR, and NOT to identify relevant articles. A secondary manual search of reference lists from selected studies was performed to capture additional eligible publications.
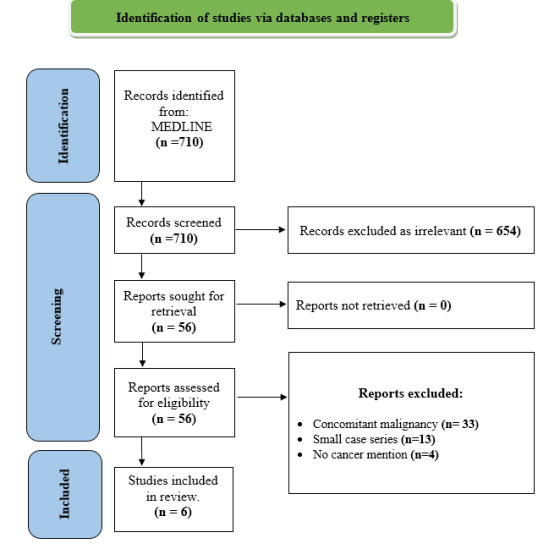
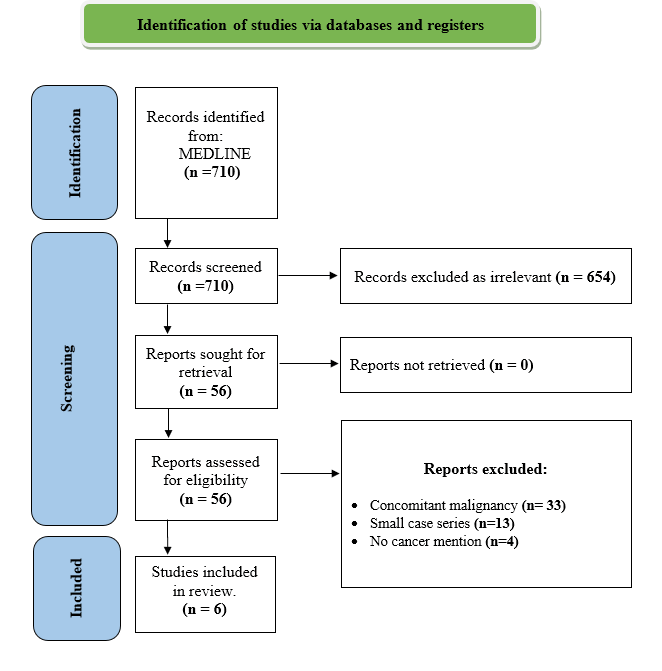
Eligibility assessment was conducted independently and in an unblinded manner by two authors (PG and CFP). The literature search process is summarized in a flow diagram (Table 1). Ultimately, six studies reporting a combined total of 67,866 patients with postoperative cancer mortality data were identified and analyzed (Table 2). These studies were published between 2010 and 2025, covering study periods from 1999 to 2023.
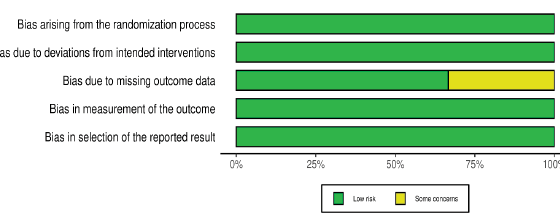
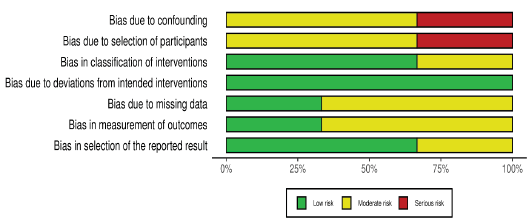
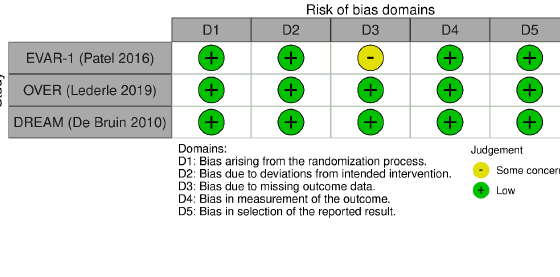
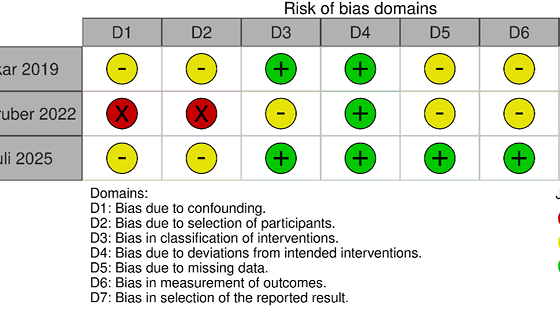
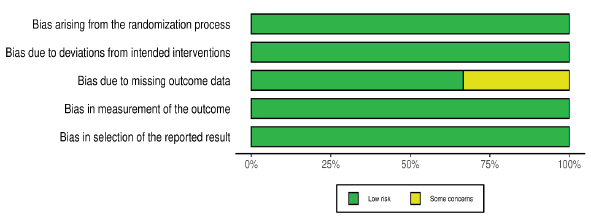
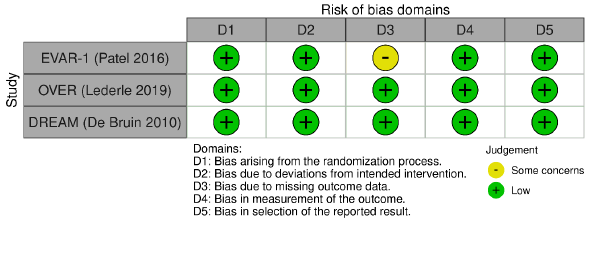
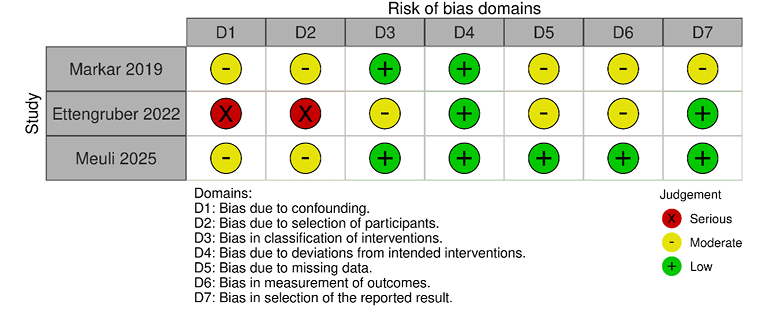
A PRISMA flow diagram summarizes the study selection process (Figure 1). The risk-of-bias assessment figures were generated as weighted bar plots (Figures 2 and 3) and “traffic light” (Figures 4 and 5) using the ROBVIS (Risk of Bias VISualization) online application in conjunction14 with the Cochrane Risk of Bias 2 (RoB 2) tool for Randomized Controlled Trials15 and the ROBINS-I V2 (Risk Of Bias In Non-randomised Studies – of Interventions, Version 2) tool for observational cohort studies.16
Eligibility, Exclusion and Inclusion Criteria
Studies were included if they reported on patients considered suitable candidates for either EVAR or OR, whether in elective or emergency (ruptured) settings. Data from all cancer-free patients were reviewed and analyzed.
Inclusion Criteria
- Studies reporting the incidence or occurrence of cancer following EVAR and/or OR
- Explicit description of cancer outcomes (preferably specifying the cancer type)
- Defined follow-up period, including time to cancer occurrence
Exclusion Criteria
- Articles not published in English
- Case reports or small series with insufficient statistical data
- Patients with concomitant malignancy or metastatic solid tumors before surgery
- Patients with a previous history of cancer
Collection of data
For each study, data were extracted regarding publication year, study duration, demographic characteristics, and relevant clinical variables, including:
- Smoking history
- Cardiac disease
- Arterial hypertension
- Chronic obstructive pulmonary disease (COPD)
- Cerebrovascular disease (CVD)
Additional parameters such as radiation exposure, number of reinterventions, and non-cancer causes of death (e.g., cardiovascular mortality) were also collected when available. Statistical comparisons focused on cancer incidence, cancer-related mortality, and overall mortality between EVAR and OR groups. Where available, hazard ratios (HR) and confidence intervals (CI) were recorded.
Weighted outcome analysis
Outcome measures were analyzed using study-size weighted pooling, where event counts were derived from each study’s sample size and reported event rate. Weighted pooled proportions were compared between EVAR and OR using two-proportion z-tests with 95 % confidence intervals (CIs). Demographics and baseline comorbidities were summarized descriptively and not weighted. Statistical significance was defined as p < 0.05.
RESULTS
A total of 710 articles were initially identified through the literature search. After screening titles, abstracts, and full texts, six studies fulfilled the inclusion criteria and were selected for final analysis.
Baseline Demographics and Comorbidities
These comprised a total of 67,866 patients (85% male), with a mean age of 72.9 ± 1.5 years. There was no significant age difference between EVAR and OR groups (p = 0.42). Among the included population, 48.4% (n=32,880) underwent EVAR, while 51.6% (n=34,986) underwent OR. The average follow-up period across studies was 10.6 years (range 1.8-15.8 years).
Baseline characteristics were largely comparable between the EVAR and OR groups, although some differences were noted. Pulmonary disease was reported in 20.1% of EVAR patients compared to 18.2% of OR patients. The DREAM trial was the only study providing detailed smoking data, reporting a prevalence of 64.2% among EVAR patients and 55.1% among those undergoing OR.
Other comorbid conditions were common across both groups. Hyperlipidemia occurred in 33.1% of EVAR patients versus 26.6% of OR patients, while diabetes mellitus was observed in 16.7% and 9.9%, respectively. Similarly, cardiovascular disease was recorded in 13.1% of EVAR and 9.1% of OR patients. Cerebrovascular disease affected 9.1% of EVAR patients but only 1.4% of those who underwent open repair. Arterial hypertension was prevalent in over half of EVAR patients (53.1%), compared with 42% of those treated with OR (Table 3).
Follow-Up and Reinterventions
The duration of follow-up varied across studies, with the EVAR-1 trial providing the longest observation period (up to 15.8 years). The overall mean follow-up across studies was approximately 10.6 years, sufficient to capture late events, including secondary malignancies and late mortality.
Follow-up duration varied among studies, with the longest follow-up reported in the EVAR-1 trial (15.8 years). Reintervention rates were significantly higher after EVAR than open repair (26.4% vs 15.2%, p < 0.001), largely due to graft-related complications such as endoleak, device migration, or limb occlusion. (Table 4). This finding was consistent across the EVAR-1, DREAM, and OVER trials and remains a well-recognized trade-off between the lower perioperative risk of EVAR and its higher long-term maintenance burden.
Mortality Outcomes
Overall mortality was significantly higher in the EVAR group, with a weighted rate of 40.6% (95% CI 39.7-41.5) compared with 35.1% (95% CI 34.1-36.2) in the OR group. The absolute difference of 5.5% (95% CI 4.3-6.7) was statistically significant (p < 0.001). This finding, while partly influenced by the large Ettengruber cohort,7 remained robust across all included studies. (Table 5).
Two of the largest randomized controlled trials – EVAR-1 and OVER – provided detailed long-term follow-up beyond eight years. Both demonstrated a trend toward increased late-onset cancer mortality in the EVAR group, although neither achieved statistical significance. In EVAR-1, cancer accounted for 28% of deaths in the EVAR group compared to 20% in the OR group (p = 0.09), while in OVER, the respective rates were 24.8% and 22.4% (p = 0.27).
Cancer Incidence and Type
For any cancer, pooling the two studies that report overall incidence7,8 yielded a higher weighted incidence after EVAR (25.97%, 95% CI 25.46-26.48) compared with open repair (22.95%; 95% CI, 22.5-23.4), corresponding to an absolute difference of 3.01% (95% CI, 2.3-3.7; p < 0.001).
Subgroup analyses from the Markar et al. study8 provided further insight into the relationship between imaging surveillance and cancer risk. When comparing EVAR patients who underwent routine CT follow-up with those who did not, the incidence of abdominal cancer was virtually identical (10.3% vs. 10.8%, p = 0.21), suggesting that CT surveillance itself was not an independent risk factor in this cohort. However, overall freedom from cancer was slightly lower among patients undergoing CT follow-up (77.5%) compared to those without (74.1%), a difference that did not reach significance (p = 0.14) (Table 6).
Lung and abdominal cancer were the predominant cancer types reported after AAA repair. When the EVAR-14 and Markar8 cohorts were combined in a weighted analysis, lung-cancer mortality was slightly higher after EVAR (6.7%; 95% CI, 6.3-7.1) than after open repair (5.7%; 95% CI, 5.4-6.0), an absolute difference of 0.98% (95% CI, 0.5-1.5) that reached statistical significance (p < 0.001). Although significant when pooled, this difference remained modest and was not significant within the individual studies (Table 7). Abdominal cancers – particularly hepatic, gastric, and colorectal – showed a more consistent association with EVAR. The multivariable analysis within the Markar cohort8 demonstrated that EVAR was associated with a 14% increased risk of abdominal cancer (HR 1.14; 95% CI, 1.03-1.27; p = 0.02) and a 9% higher overall cancer incidence (HR 1.09; 95% CI, 1.02-1.17; p = 0.01) compared with open repair.
However, more contemporary large-scale studies, including that of Meuli et al. (2025), have not confirmed a significant difference in cancer incidence between patients undergoing endovascular versus open aneurysm repair. Specifically, the study evaluated a secondary endpoint and found no difference in 10-year incidence of solid malignant tumors between OSR and EVAR (OSR: 18.6% vs EVAR: 20.5%; P=0.35) in their weighted analysis.
DISCUSSION
This pooled analysis of more than 67,000 patients provides contemporary evidence on long-term outcomes after endovascular (EVAR) versus open abdominal aortic aneurysm repair (OR). Although baseline characteristics were broadly comparable, EVAR patients exhibited slightly higher rates of cardiopulmonary comorbidities, reflecting selection of higher-risk individuals for the endovascular approach. Advancing age inherently increases the likelihood of genetic mutations, and shared risk factors -particularly smoking and chronic obstructive pulmonary disease (COPD) – may predispose these patients to both diseases.10,17
The most novel aspect of this analysis concerns the potential association between EVAR and increased cancer incidence. When data from Markar8 and Ettengruber7 were pooled, EVAR was associated with a 3% absolute increase in overall cancer incidence (25.9% vs 22.9%, p<0.001).7,8 These observations raise important questions regarding possible etiologic mechanisms, including chronic inflammation from the implanted endograft, local hemodynamic or ischemic effects, and repeated radiation exposure from postoperative imaging.
Radiation exposure from intraoperative fluoroscopy and postoperative CT surveillance remains a key concern in EVAR patients11,12,13 Arterial hypertension, present in 53.1% of EVAR cases, often requires higher contrast doses, indirectly increasing radiation exposure – a recognized stochastic carcinogenic risk.18 Although standard EVAR involves modest radiation, repeated CT follow-up markedly increases cumulative exposure.19 Monte Carlo models estimate that about one-third of lifetime cancer risk after EVAR arises from combined pre-, intra-, and postoperative imaging. 20 More intensive CT regimens (biannual vs. annual) nearly double attributable cancer risk. While Markar et al.8 found no significant difference in cancer incidence among patients undergoing CT surveillance, recent dosimetric studies confirm that cumulative exposure remains clinically relevant.21 Organ-specific analyses show that the liver, stomach, and colon receive the highest doses, though related cancer mortality remains below 0.1%. Bone marrow exposure—mainly from fluoroscopy—may contribute most to long-term stochastic effects.12,22
The present analysis benefits from inclusion of large randomized trials with extended follow-up, ensuring adequate power to detect late events. However, heterogeneity in study design, imaging protocols, and cancer ascertainment methods introduces potential bias. The lack of granular data on smoking history, radiation dose, and cancer subtype limits mechanistic interpretation. Additionally, despite adjustment in individual studies, residual confounding cannot be excluded.
This review has several limitations. It was not a formal meta-analysis; results were derived from sample-size weighting without adjustment for study heterogeneity. Reported p-values are descriptive and should be interpreted cautiously. Included studies varied in design, population risk, and follow-up protocols, with incomplete data on confounders such as smoking, radiation dose, and cancer type. Direct quantification of radiation exposure was not possible, and publication bias cannot be excluded.
CONCLUSION
In conclusion, long-term data indicate that while EVAR remains less invasive and initially safer than open repair, it carries a greater burden of reinterventions and possibly higher late mortality. The observed association between EVAR and increased cancer incidence is modest, inconsistent across studies, and likely multifactorial. Ongoing surveillance of contemporary EVAR cohorts, particularly with modern low-dose imaging protocols, is essential to clarify whether these associations persist in current practice.
REFERENCES
- Ahn S, Min JY, Kim HG, Mo H, Min SK, Min S, et al. Outcomes after aortic aneurysm repair in patients with a history of cancer: a nationwide database analysis. BMC Surg. 2020;20(1):85.
- Kumar R, Dattani N, Asaad O, Bown MJ, Sayers RD, Saratzis A. Meta-analysis of outcomes following aneurysm repair in patients with synchronous intra-abdominal malignancy. Eur J Vasc Endovasc Surg. 2016;52(6):747-756.
- Jetty P, Husereau D. Trends in the utilization of endovascular therapy for elective and ruptured abdominal aortic aneurysm procedures in Canada. J Vasc Surg. 2012;56(6):1518-1526.
- Patel R, Sweeting MJ, Powell JT, Greenhalgh RM; EVAR Trial Investigators. Endovascular versus open repair of abdominal aortic aneurysm in 15 years’ follow-up of the UK endovascular aneurysm repair trial 1 (EVAR trial 1): a randomized controlled trial. Lancet. 2016;388:2366-2374.
- Lederle FA, Freischlag JA, Kyriakides TC, Padberg FT, Matsumura JS, Kohler TR, et al. Long-term comparison of endovascular and open repair of abdominal aortic aneurysm. N Engl J Med. 2012;367(21):1988-1997.
- De Bruin JL, Baas AF, Buth J, Prinssen M, Verhoeven EL, Cuypers PW, et al; DREAM Study Group. Long-term outcome of open or endovascular repair of abdominal aortic aneurysm. N Engl J Med. 2010;362(20):1881-1889.
- Ettengruber A, Epple J, Schmitz-Rixen T, Böckler D, Grundmann RT. Long-term outcome and cancer incidence after abdominal aortic aneurysm repair. Langenbecks Arch Surg. 2022;407(8):3691-3699.
- Markar SR, Mackenzie H, Karthikesalingam A, Holt PJ, Thompson MM, Loftus IM, et al. A population-based cohort study examining the risk of abdominal cancer after endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2019;69(6):1776-1785.e2.
- Spencer C, Jamrozik K, Kelly S, Bremner P, Norman P. Is there an association between chronic lung disease and abdominal aortic aneurysm expansion? ANZ J Surg. 2003;73(10):787-789.
- Blochle R, Lall P, Cherr GS, Harris LM, Dryjski ML, Hsu HK, et al. Management of patients with concomitant lung cancer and abdominal aortic aneurysm. Cardiol Res Pract. 2011;2011:516146.
- Motaganahalli R, Martin A, Feliciano B, Murphy MP, Slaven J, Dalsing MC. Estimating the risk of solid organ malignancy in patients undergoing routine computed tomography scans after endovascular aneurysm repair. J Vasc Surg. 2012;56(4):929-937.
- Kramer R, Khoury HJ, Vieira JW. CALDose_X: a software tool for the assessment of organ and tissue absorbed doses, effective dose, and cancer risks in diagnostic radiology. Phys Med Biol. 2008;53:6437-6459.
- Saltybaeva N, Martini K, Frauenfelder T, Alkadhi H. Organ dose and attributable cancer risk in lung cancer screening with low-dose computed tomography. PLoS One. 2016;11(5):e0155722.
- McGuinness LA, Higgins JPT. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res Synth Methods. 2021;12(1):55-61.
- Sterne JAC, Savović J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ. 2019;366:l4898.
- Sterne JA, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. 2016;355:i4919
- Goodney PP, Tavris D, Lucas FL, Gross T, Fisher ES, Finlayson SRG. Causes of late mortality after endovascular and open surgical repair of infrarenal abdominal aortic aneurysms. J Vasc Surg. 2010;51(6):1340-1347.e1.
- Brambilla M, Cerini P, Lizio D, Vigna L, Carriero A, Fossace R. Cumulative radiation dose and radiation risk from medical imaging in patients subjected to endovascular aortic aneurysm repair. Radiol Med. 2015;120(6):563-570.
- Singh B, Andersson M, Edsfeldt A, Sonesson B, Gunnarsson M, Dias NV. Estimation of the added cancer risk derived from EVAR and CTA follow-up. J Endovasc Ther. 2023;30(6):1021-1030.
- Blaszak MA, Juszkat R. Monte Carlo simulations for assessment of organ radiation doses and cancer risk in patients undergoing abdominal stent-graft implantation. Eur J Vasc Endovasc Surg. 2014;48(1):23-28
- Blakely EA. Biological effects of cosmic radiation: deterministic and stochastic. Health Phys. 2000;79(5):495-506.
- Meuli L, Zimmermann A, Petersen JK, Fosbøl EL, Dabravolskaitė V, Makaloski V, et al. Risk stratification and treatment selection in patients with asymptomatic abdominal aortic aneurysms. Eur J Vasc Endovasc Surg. 2021;61(2):275-283
{kind=link}
{kind=link}
{kind=link}
{kind=link}