Simultaneous Acute Thrombosis of Bilateral Popliteal Artery Aneurysms Causing Acute Ischemia of both lower limbs

| Available Online: | March, 2026 |
| Page: | 37–40 |
Author for correspondence:
Nikolaos Kontopodis
Vascular Surgery Unit, Department of Cardiothoracic and Vascular Surgery, University Hospital of Heraklion, Medical School, University of Crete, Voutes, Heraklion 71110, Greece
E-mail: nkontopodis@uoc.gr
doi: 10.59037/rx2t7085
eISSN: 2732-7167 / 2026 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Michalis Pesmatzoglou1, Nikolaos Kontopodis1, Elias Kehagias2, Konstantinos Litinas1, Ifigeneia Tzartzalou1, Alexandros Liamis1, Alexandros Kafetzakis1, Christos V. Ioannou1
1 Vascular Surgery Unit, Department of Vascular and Cardiothoracic Surgery, University Hospital of Heraklion, Medical School,
University of Crete, Heraklion, Greece
2 Interventional Radiology Unit, Department of Medical Imaging, University Hospital of Heraklion, Medical School, University of
Crete, Heraklion, Greece
Full Text
Gallery
Full Text
Abstract:
Purpose: Popliteal artery aneurysms (PAAs) are rare, typically asymptomatic lesions that are managed electively. Acute thrombosis, however, poses an immediate threat to limb viability, necessitating prompt diagnosis and intervention. We report a rare case of simultaneous bilateral PAA thrombosis presenting with acute limb ischemia.
Case report: A 60-year-old male presented to the emergency department with acute bilateral lower limb pain and numbness due to simultaneous thrombosis of bilateral PAAs, resulting in acute limb ischemia. Aneurysmal disease involving both the left common iliac and common femoral arteries, with significant intramural thrombus resulting in >60% stenosis, posed substantial challenges to management. A hybrid endovascular and open surgical approach was selected to address all aneurysms concurrently. To our knowledge, this is the first reported case of simultaneous bilateral PAA thrombosis causing acute limb ischemia.
Conclusion: This complex presentation underscores the need for meticulous diagnostic and therapeutic strategies to achieve optimal outcomes.
Keywords: popliteal artery aneurysm, bilateral thrombosis, acute limb ischemia, case report
INTRODUCTION
Popliteal artery aneurysms (PAAs) are the most common peripheral artery aneurysms, comprising approximately 85% of cases.1,2 About 80% of PAAs are asymptomatic at diagnosis but acute thrombosis can cause limb-threatening ischemia, requiring urgent intervention.2 This report presents a unique case of simultaneous acute thrombosis of bilateral PAAs causing bilateral lower limb ischemia, a presentation not previously documented in the literature. This case is reported per CARE guidelines.
CASE REPORT
Patient Information: A 60-year-old male heavy smoker presented to the emergency department with acute-onset bilateral lower limb pain and numbness. No history of thrombophilia, genetic disorders, autoimmune conditions or relevant family history was identified.
Clinical Findings: Both lower limbs appeared pale with cold feet and delayed capillary refill (>3 seconds). The patient reported numbness with no sensory or motor deficits. Femoral pulses were palpable bilaterally while more distal pulses were absent. Doppler ultrasound showed weak monophasic signals at the malleolar level, with an ankle-brachial index of 0.2 bilaterally. Thrill and bruit were present over the left femoral artery. These findings indicated Rutherford Grade I (viable) acute ischemia bilaterally.
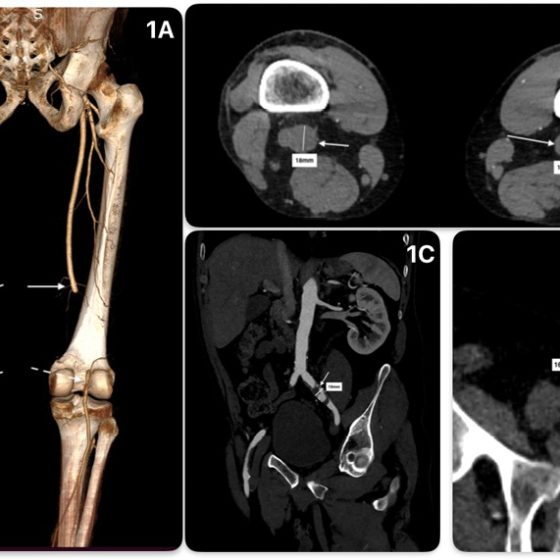
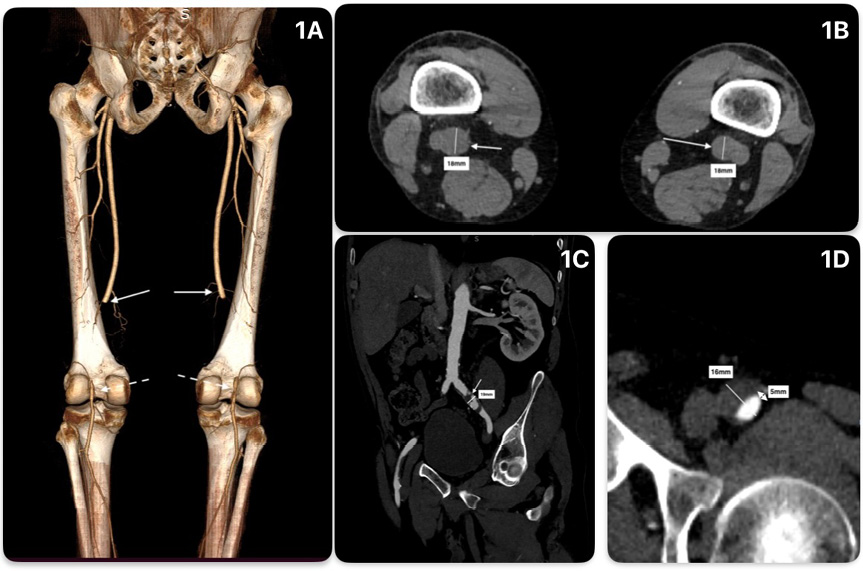
Diagnostic Assessment: Laboratory tests were unremarkable. Computed tomography angiography (CTA) of the thoracoabdominal aorta and lower limbs revealed occluded bilateral PAAs (maximum diameter: 18 mm bilaterally) with good three-vessel tibial runoff (Figure 1A, B). Additionally, left common iliac (19 mm) and common femoral (16 mm) artery aneurysms were identified, each with thrombus causing >60% stenosis (Figure 1C, D).
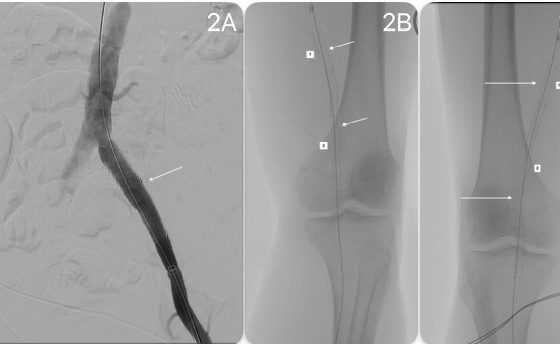
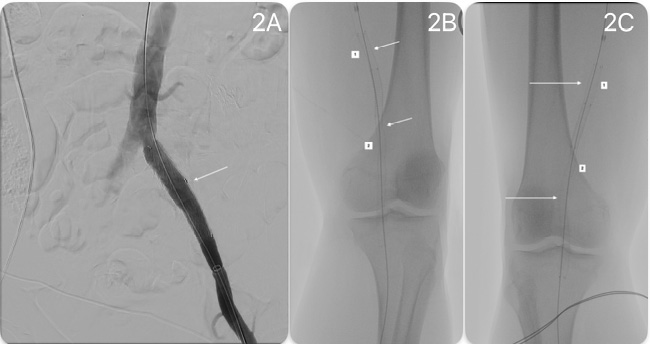
Therapeutic Intervention: Given the concurrent aneurysms, a hybrid approach was selected, under spinal anesthesia, in the angiography suite. Open aneurysmatectomy and interposition grafting of the left common femoral artery aneurysm was performed (8-mm Dacron graft), Retrograde access through the graft facilitated insertion of a 16x12x70-mm iliac limb extension stent-graft (W. L. GORE & Associates, Flagstaff, Ariz), delivered through a 12x33mm sheath to exclude the left common iliac artery aneurysm (Figure 2A). Antegrade access through the left SFA (direct vision, 8x11mm sheath) and right common femoral artery (percutaneous access, ProGlide closure device) enabled bilateral PAA exclusion with Viabahn® (W. L. GORE & Associates, Flagstaff, Ariz) stent-grafts (7x150mm and 8x75mm bilaterally) (Figure 2 B, C). Catheterization of the occluded PAAs was straightforward bilaterally, confirming the fact that thrombosis was acute. The stent grafts were deployed first distally (2cm below knee crease) and then proximally (above-the-knee) ensuring adequate sealing.
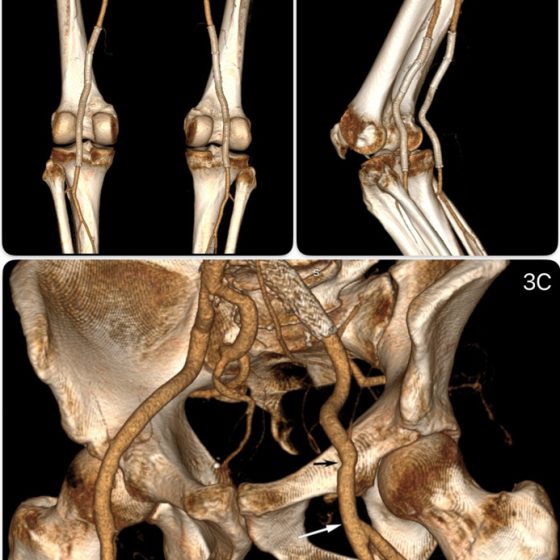
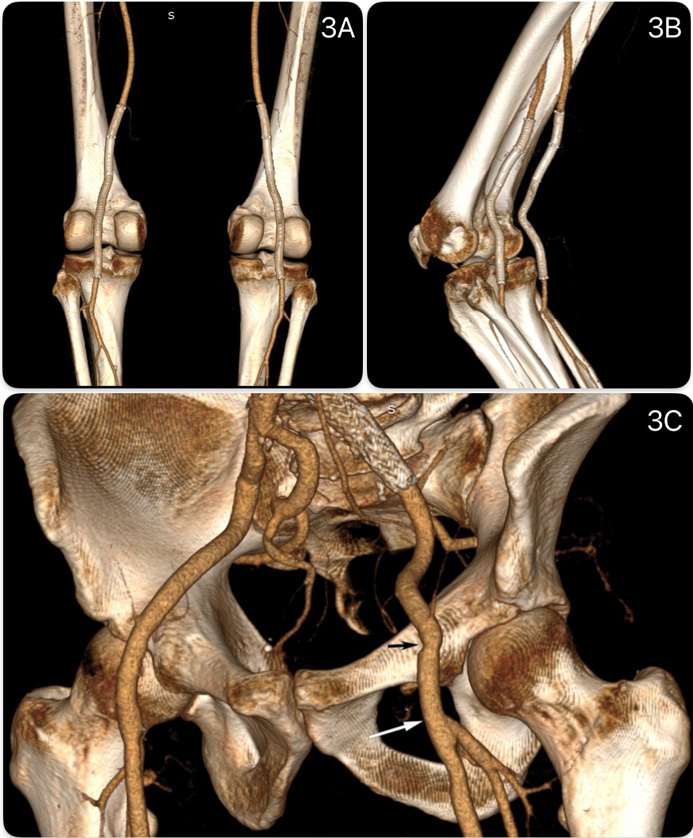
Follow-up and Outcomes: Immediately postoperatively, palpable distal pulses were restored and ABI normalized bilaterally. The postoperative course was uneventful. The patient was discharged on day 8, with antiplatelet and anticoagulant therapy and genetic screening recommendations. One-month CTA (knee extended/flexed) confirmed optimal stent-graft positioning (Figure 3A, B). Left interposition graft and both SFA and PFA remained patent (Figure 3C). At 3-months, clinical examination showed palpable distal pulses and ABI 1.0 bilaterally. Mid- and long-term follow-up outcomes are not currently available and they are anticipated.
DISCUSSION
Acute PAA thrombosis is a limb-threatening emergency, with amputation rates in symptomatic cases up to 25%.3
No universal consensus exists on the optimal PAA management.3,4 The 2022 SVS guidelines recommend open repair for asymptomatic patients with >5 years life expectancy and suitable vein conduits, while acute ischemia management depends on ischemia grade.5 Adequate inflow and outflow are critical for durable patency in both techniques.3, 4 Recent literature suggests progressively increased rates of endovascular interventions compared to open surgery.6
Here, the CFA aneurysm mandated open reconstruction, whereas the common iliac artery [CIA] and bilateral PAAs were amenable to either open or endovascular approach. Good tibial runoff was considered favorable in order for the patient to undergo endovascular treatment (Figure 1A).
The chosen hybrid approach, open femoral repair combined with endovascular repair of the left CIA and bilateral PAAs, optimized both inflow and outflow, enhancing long-term patency, while reducing operative time and perioperative morbidity compared to fully open repair.
In the literature, endovascular repair yields outcomes comparable to open reconstruction, in acute settings.2 Antonello et al found no significant difference in 4-year patency or limb salvage rates between open (OPAR) and endovascular (EPAR) reconstruction, with EPAR offering shorter hospital stay and faster recovery.7 Recent reviews highlight EPAR benefits, including reduced operative time, minimal blood loss, fewer wound infections and avoidance of general anesthesia.4 A large study of 1159 PAA showed no difference in reintervention rates or major amputation, at 1-, 3- and 5- years, between OPAR and EPAR, even with vein conduits.8
EPAR risks include stent-graft occlusion, fracture, migration or endoleak, largely due to repetitive knee motion.4
The Viabahn® stent-graft offers flexibility and durability, via its thin, heparin-coated PTFE lining and self-expanding nitinol framework, with patency and limb salvage rates comparable to OPAR.9 Post-operative CTA (knee flexed/extended) confirmed no excessive angulation, fracture or migration (Figure 3).
Approximately one third of PAA patients are ineligible for EPAR, and another 23% have significant contraindications. Therefore, strict adherence to Instructions for Use (IFU) is critical for success.10
Dual antiplatelet therapy (DAPT) is commonly recommended post-EPAR, with potential transition to single therapy.11 When anticoagulation is indicated, triple therapy may be considered (DAPT plus warfarin, INR 2.0-3.0), balancing bleeding risk.12 Guidelines for infrainguinal endovascular reconstruction suggest low-dose rivaroxaban twice daily plus aspirin] or DAPT for at least six months, while not addressing specifically post-EPAR.13 Lacking specific EPAR guidance and given acute ischemia with multiple stents placed, we opted for lifelong aspirin 100mg daily and rivaroxaban 20mg daily.
This represents the first reported case of simultaneous bilateral acute PAA thrombosis causing bilateral limb ischemia, illustrating the complexity of managing multiple aneurysms and the value of individualized hybrid strategies.
CONCLUSION
Popliteal artery aneurysms are rare, often bilateral and asymptomatic, typically managed electively. Acute thrombosis is a major complication, causing limb-threatening ischemia, requiring prompt treatment. Simultaneous, acute thrombosis of bilateral PAAs, resulting in bilateral ischemia, is exceptionally uncommon. This case report underscores the complexity of such presentations, emphasizing critical role of meticulous pre-procedural planning to optimize outcomes.
REFERENCES
- Demas N, Saha SP. Popliteal artery aneurysm repair-A single center experience. Asian Cardiovasc Thorac Ann.2024;32:157-163.
- Aragão JA, de Miranda FGG, Aragão ICS, Aragão FMS, Reis FP. Treatment of bilateral popliteal artery aneurysms. J Vasc Bras. 2019 Nov 29;19:e20180142.
- Ripepi M, Gibello L, Ferrero E, Scevola M, Manzo P, Varetto G et al. Open Versus Endovascular Repair of Patent Popliteal Artery Aneurysms in an Elective Setting: A Multicenter Retrospective Study with Long-Term Follow-Up. Ann Vasc Surg. 2025;117:64-71.
- Tian Y, Yuan B, Huang Z, Zhang N. A Comparison of Endovascular Versus Open Repair of Popliteal Artery Aneurysms: An Updated Meta-Analysis. Vasc Endovascular Surg. 2020;54:355-361.
- Farber A, Angle N, Avgerinos E, Dubois L, Eslami M, Geraghty P, et al. The Society for Vascular Surgery clinical practice guidelines on popliteal artery aneurysms. J Vasc Surg. 2022;75(1S):109S-120S.
- Wrede A, Wiberg F, Acosta S. Increasing the Elective Endovascular to Open Repair Ratio of Popliteal Artery Aneurysm. Vasc Endovascular Surg. 2018;52:115-123.
- Antonello M, Frigatti P, Battocchio P, Lepidi S, Cognolato D, Dall’Antonia A, et al. Open repair versus endovascular treatment for asymptomatic popliteal artery aneurysm: results of a prospective randomized study. J Vasc Surg. 2005;42:185-93.
- Satam K, Brahmandam A, Zheng X, Mao J, Goodney P, Ochoa Chaar CI. Long-term outcomes of elective endovascular vs open repair of popliteal artery aneurysms in the VISION database. J Vasc Surg. 2025;81:672-681.
- Patel SR, Hughes CO, Jones KG, Holt PJ, Thompson MM, Hinchliffe RJ, et al. A Systematic Review and Meta-analysis of Endovascular Popliteal Aneurysm Repair Using the Hemobahn/Viabahn Stent-Graft. J Endovasc Ther. 2015;22:330-7.
- Hellwig K, Hoffmann L, Rother U, Meyer A, Lang W, Schmid A. Eligibility of Endovascular Repair for Popliteal Artery Aneurysms According the Instructions for Use. Ann Vasc Surg. 2020;67:370-375.
- van Leeuwen GL, Baggel S, Tielliu IFJ, Schuurmann RCL, van Walraven LA, de Vries JPM. Editor’s Choice – Long Term Follow-Up after Endovascular Popliteal Artery Aneurysm Repair: A Two Centre, Retrospective Cohort Study (1998 – 2023). Eur J Vasc Endovasc Surg. 2025 Oct;70(4):483-489. doi: 10.1016/j.ejvs.2025.04.041. Epub 2025 Apr 26. PMID: 40294783.
- Ullery BW, Tran K, Itoga N, Casey K, Dalman RL, Lee JT. Safety and efficacy of antiplatelet/anticoagulation regimens after Viabahn stent graft treatment for femoropopliteal occlusive disease. J Vasc Surg. 2015 Jun;61(6):1479-88. doi: 10.1016/j.jvs.2014.12.062. Epub 2015 Feb 19. PMID: 25704407.
- Twine CP, Kakkos SK, Aboyans V, Baumgartner I, Behrendt CA, Bellmunt-Montoya S, Jilma B, Nordanstig J, Saratzis A, Reekers JA, Zlatanovic P; ESVS Guidelines Committee; Antoniou GA, de Borst GJ, Bastos Gonçalves F, Chakfé N, Coscas R, Dias NV, Hinchliffe RJ, Kolh P, Lindholt JS, Mees BME, Resch TA, Trimarchi S, Tulamo R, Vermassen FEG, Wanhainen A; Document Reviewers; Koncar I, Fitridge R, Matsagkas M, Valgimigli M. Editor’s Choice – European Society for Vascular Surgery (ESVS) 2023 Clinical Practice Guidelines on Antithrombotic Therapy for Vascular Diseases. Eur J Vasc Endovasc Surg. 2023 May;65(5):627-689. doi: 10.1016/j.ejvs.2023.03.042. Epub 2023 Apr 3. PMID: 37019274.
Figure 1: A. 3-dimensional reconstruction of the pre-operative CT scan, in which a posterior view is demonstrated, showing the occluded popliteal arteries (solid white arrows show the proximal and dashed arrows the distal extent of the occlusions) B. Axial CT views at the level of the knee crease showing bilateral 18mm occluded popliteal artery aneurysms C. Coronal view showing the left common iliac artery aneurysm (solid white arrow) with a significant amount of intraluminal thrombus. D. Axial view showing the left common femoral artery aneurysm with a significant amount of intraluminal thrombus, leaving around 30% of residual patent lumen (white arrow).
 Figure 2: A. Intraoperative angiography showing successful exclusion of the left common iliac artery aneurysm with the deployment of an iliac limb extension (white arrow) B. Intraoperative x-ray indicating successful deployment of the 2 Viabahn® stent-grafts on the left side (1 for the proximal/8x75mm and 2 for the distal/7x150mm stents), which were deployed from distal to proximal. C. Same for the right side.
Figure 2: A. Intraoperative angiography showing successful exclusion of the left common iliac artery aneurysm with the deployment of an iliac limb extension (white arrow) B. Intraoperative x-ray indicating successful deployment of the 2 Viabahn® stent-grafts on the left side (1 for the proximal/8x75mm and 2 for the distal/7x150mm stents), which were deployed from distal to proximal. C. Same for the right side.
Figure 3: A. 3-dimensional reconstruction of postoperative CT angiography with limbs in extension B. Same with limbs in flexion. C. The surgical graft is shown with the black arrow indicating the level of the proximal and the white arrow the level of the distal anastomosis.
{kind=link}
{kind=link}
{kind=link}