Left Superior Gluteal Pelvic Escape Point Associated with Nonthrombotic Iliac Vein Compression Syndrome
| Available Online: | March, 2026 |
| Page: | 41 |
Author for correspondence:
Phong T. Le, MD, PhD
Department of Vascular Surgery, Cho-Ray Hospital,
201B Nguyen Chi Thanh, Hochiminh City 72713, Vietnam
E-mail: phonglechir@gmail.com
doi: 10.59037/xkqxve48
eISSN: 2732-7167 / 2026 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Van-Nut Lam, Nha-Truc N Lam, Thanh-Phong Le
Cho-Ray Hospital, Ho Chi Minh City
Full Text
Gallery
Full Text
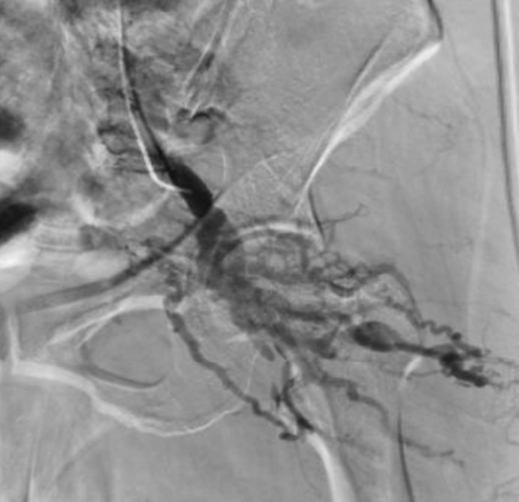
Figure 1: Descending venography of the left internal iliac vein demonstrating voluminous reflux arising from the left superior gluteal vein (SGV), feeding numerous varicosities of the ipsilateral buttock
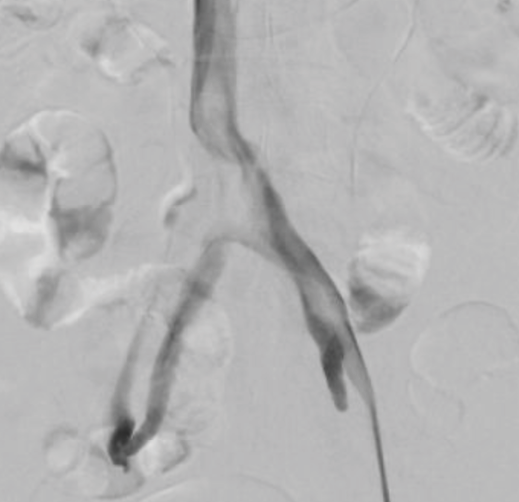
Figure 2: Nonthrombotic left iliac vein compression syndrome (NTIVC)
A 52-year-old female presented with pelvic vein disorders (PeVD) and symptomatic extensive atypical varicosities on the left buttock, posterior thigh, and lower leg. Duplex ultrasound (DUS) revealed reflux originating from a pelvic vein superior to the piriformis muscle. Descending venography of the left internal iliac vein demonstrated voluminous reflux arising from the left superior gluteal vein (SGV), feeding numerous varicosities of the ipsilateral buttock (Figure 1). This was associated with a nonthrombotic left iliac vein compression syndrome (NTIVC) (Figure 2). The patient was therefore classified as S2,3bV2,3bPLCIV,O,NT; LPELV,R,NT; [L]C2sEsieAs,dPo(CIV),r(PELV,NSV) according to the Symptoms-Varices-Pathophysiology and Clinical-Etiology-Anatomy-Pathophysiology classifications.
Venographic description of the superior gluteal pelvic escape point (SGP) has been rarely reported. The SGV typically enters the pelvis at an acute, superior angle, and is deeply encased by surrounding gluteal muscle. Consequently, blood outflow from high-pressure pelvic veins into the SGV is restricted compared to other internal iliac vein branches. The occurrence of the SGP was potentially triggered by anatomical variants and NTIVC.
A combination of foam sclerotherapy and coil embolization, along with recanalization of the left common iliac vein, has been performed. Follow-up visits extending up to eight years post-intervention have consistently demonstrated significant clinical improvements, a patent iliac stent, and the absence of pre-existing reflux from SGP on DUS. The Patient consented to the publication.