Bridging the gap: Short prosthetic graft adjunctive conduit for primary brachiocephalic fistula construction

| Available Online: | March, 2026 |
| Page: | 42–43 |
Author for correspondence:
Kate Tabaku, MD
Department of Vascular Surgery, General University Hospital
of Patras, Patras Medical School, Patras, Greece
E-mail: katetabaku@gmail.com
doi: 10.59037/4hjwk830
eISSN: 2732-7167 / 2026 Hellenic Society of Vascular and
Endovascular Surgery Published by Rotonda Publications
All rights reserved. https://www.heljves.com
1 Department of Vascular Surgery, General University Hospital of Patras, Patras Medical School, Patras, Greece
2 Department of Nephrology, General Hospital of Patras ‘St Andrew’, Patras, Greece
3 Department of Radiology, General University Hospital of Patras, Patras Medical School, Patras, Greece
Full Text
Gallery
Full Text
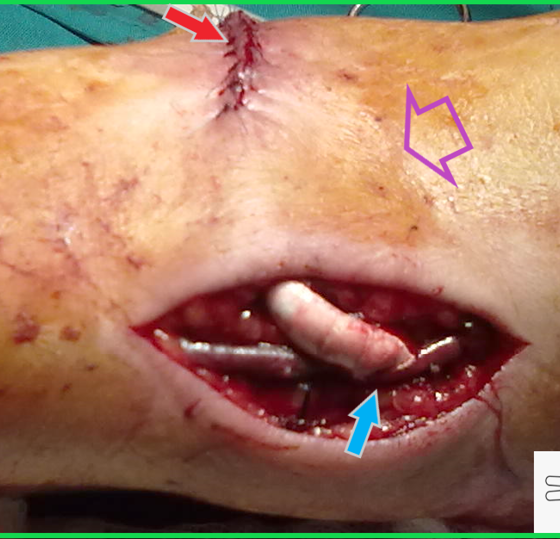
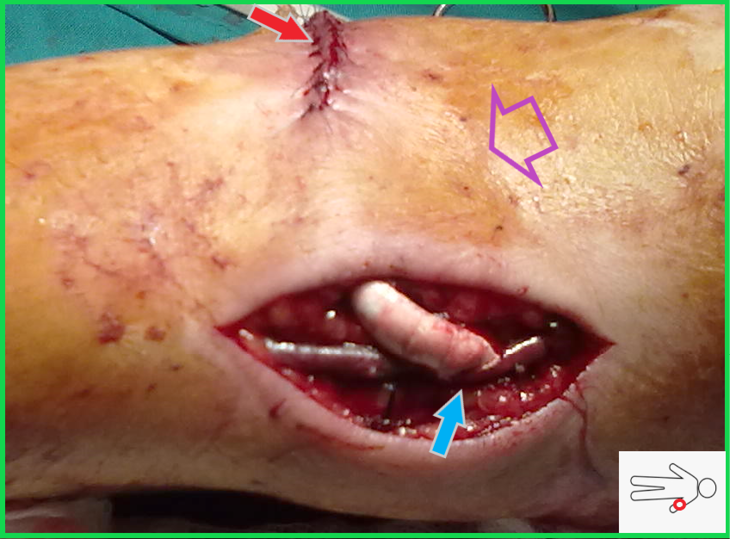
Figure 1. A short conical synthetic graft bridged the gap between the left brachial artery and the cephalic vein (Purple arrow: the antecubital fossa, red arrow: the site of arterial anastomosis-not seen as skin incision is closed, light blue arrow: the venous anastomosis)
A 75-year-old-male diabetic patient with end-stage renal disease was scheduled for left upper arm arteriovenous fistula (AVF) creation. He initiated dialysis via a right-sided tunneled central catheter. Preoperative ultrasound mapping revealed suitable vessels at the elbow level. Unfortunately, the median cubital vein was absent and the distance between the brachial artery and cephalic vein was about 4cm. We proceeded with a bridging graft between these vessels with end-to-side anastomoses. We preferred to use the conic part of a 4-7 tapered polytetrafluoroethylene (PTFE) graft (Gore Intering; W.L. Gore & Associates, Flagstaff, AZ, USA) (Figure 1). The upper arm cephalic matured adequately and the cannulation was normal for the next 9 years, when the patient died.
An entirely autologous construction would require wide mobilization of the upper arm cephalic vein with longer skin incisions, as the forearm cephalic vein was diminutive. In this case, the autologous anastomosis would rather be performed above the elbow resulting in a reduced functional cannulation length. This pushed the decision towards the use of a short graft, having in mind the disadvantages of a non-autologous access. Reviewing the English literature, we were not able to find a similar approach in primary AVF procedures. However, use of short PTFE grafts has been widely used in redo operations to correct AVF stenoses, bleeding, pseudoaneurysms, high-flow AVFs and steal syndrome1,2,3 with satisfactory results.
REFERENCES
- Georgiadis GS, Lazarides MK, Lambidis CD, Panagoutsos SA, Kostakis AG, Bastounis EA, Vargemezis VA. Use of short PTFE segments (<6 cm) compares favorably with pure autologous repair in failing or thrombosed native arteriovenous fistulas. J Vasc Surg. 2005 Jan;41(1):76-81.
- Papadoulas S, Mulita F, Theodoropoulou T, Dousdampanis P. Short interposition grafting for dialysis-access steal syndrome treatment. BMJ Case Rep. 2022 Feb 28;15(2):e248446.
- Papadoulas SI, Kouri N, Tsimpoukis A, Kitrou P, Papasotiriou M, Nikolakopoulos KM, Moulakakis KG. Treatment options for dialysis access steal syndrome. Pol J Thorac Cardiovasc Surg. 2022 Sep;19(3):141-145.
{kind=link}