
How I Did It: Technique for four-fenestrated Physician-modified Endograft to Treat Complex Abdominal Aortic Aneurysms using the Bolton Treo

| Available Online: | October, 2025 |
| Page: | 125–136 |
Author for correspondence:
Konstantinos Moulakakis
First Department of Vascular Surgery, University of Athens Medical School, Attikon Hospital, Athens, Greece
E-mail: konmoulakakis@yahoo.gr
doi: 10.59037/yh4s2p51
ISSN 2732-7175 / 2025 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Konstantinos G. Moulakakis,* Aristotelis Yfantis,* Georgios Plakas, Christos Pitros, Constantine N. Antonopoulos, Georgios S. Sfyroeras, Andreas M. Lazaris, John D. Kakisis
1st Department of Vascular Surgery, Medical School, National and Kapodistrian University of Athens, Attikon University Hospital,
Athens, Greece
*The first two authors have contributed equally to the writing of the manuscript
Full Text
Gallery
Full Text
INTRODUCTION
Endovascular repair has become the preferred treatment method for abdominal aortic aneurysms (AAAs) in anatomically suitable patients, offering reduced perioperative morbidity and mortality rates compared to open surgery.1 However, a significant percentage of patients present with complex abdominal aortic aneurysms (cAAA) including juxtarenal, pararenal, paravisceral and type IV thoracoabdominal aneurysmswhere an insufficient infrarenal sealing zone prevents standard endovascular aneurysm repair (EVAR). To achieve a sufficient proximal seal, it is necessary to extend the landing zone above the renal and, in certain cases, the mesenteric vessels.
Fenestrated and branched endovascular aortic repair (FEVAR/BEVAR) using custom made devices (CMDs) has emerged as a widely accepted approach for these complex anatomies. Contemporary CMD FEVAR/BEVAR series demonstrate high technical success rates and favorable perioperative outcomes, reflecting improved device design and increasing operator experience.2 Long-term and midterm studies further report acceptable survival, sustained aneurysm exclusion, and durable target vessel patency in pararenal and thoracoabdominal aneurysms treated with CMDs.3 Multicenter and multicohort evaluations indicate that CMD FEVAR/BEVAR can consistently achieve technical success across experienced centers when appropriate planning and imaging protocols are applied.3 Furthermore, the use of CMDs has proven effective in both elective and high-risk patient cohorts with juxtarenal aneurysms, showing better outcomes compared to those undergoing open repair.4
Despite these advances, CMD FEVAR/BEVAR is subject to inherent limitations. The time required for device manufacturing introduces a significant delay from the indication to implantation, rendering CMDs less practical for urgent or emergency indications. Access to CMD programs can be restricted by geographical location, reimbursement policies, device availability, and anatomical constraints related to device design. These factors continue to challenge seamless customizations for all patients. These practical barriers create a clinical gap, particularly in patients with symptomatic, rapidly expanding, or ruptured complex aortic aneurysms. Physician-modified endografts (PMEGs) have been developed to address this gap. PMEGs are created by back-table modification of commercially available endografts to incorporate custom fenestrations aligned with target vessels. Since the first descriptions of physician-modified techniques, numerous centers have adopted PMEG workflows to treat complex infrarenal, juxtarenal, and pararenal aneurysms when CMDs are not readily available or urgent repair is indicated.5,6 Early observational studies and systematic reviews indicate a high rate of technical success and acceptable short-term efficacy, although significant heterogeneity in reporting standards and device platforms has impeded outcome interpretation.6
More recent large observational cohorts and registry data have provided important evidence supporting PMEG feasibility in a broader range of clinical contexts. A multicenter PMEG study including over 1,200 patients demonstrated high technical success and encouraging early outcomes across elective, symptomatic, and ruptured complex aneurysm cohorts.7 Longterm follow-up studies conducted at high-volume centers further demonstrate durable exclusion and satisfactory target vessel patency up to five years following implantation.8
As PMEG adoption has expanded, attention has increasingly focused on the technical challenges associated with these techniques. These include meticulous preoperative planning, precise fenestration alignment, device re-sheathing, and reliable target vessel cannulation, especially in the presence of severe aortic angulation or tortuosity.9 Surveys of global practice patterns confirm substantial variability in indications, planning strategies, and device platforms, reflecting the absence of standardized workflows and dependence on individual operator experience.9 In response to this variation, recent multicenter initiatives have evaluated structured four-fenestration workflows, demonstrating promising early outcomes while highlighting the importance of reproducible planning and execution principles.10
The selection of an appropriate device is pivotal in assessing the feasibility of PMEG. The Terumo Aortic TREO endograft has emerged as a particularly versatile platform for physician modification due to features such as a long main body, wide stent-to-stent spacing, controlled deployment, and capacity for partial deployment and re-sheathing. Dedicated reports describe TREO modification for incorporation of up to four fenestrations in juxtarenal and pararenal aneurysms, even in emergency situations.11,12 Simulation studies further support the geometric compatibility of four fenestrated PMEG design with the use of TREO endograft, suggesting potential advantages in planning and structural characteristics.13
Despite increasing evidence supporting the use of PMEGs, it remains an off-label technique, and its success significantly depends on patient selection, detailed planning, and operator expertise. Experts agree that PMEGs should be performed in specialized centers characterized by robust governance, a high volume of cases, and experience with complex endovascular aortic repair.
This article describes a reproducible technique for the creation and implantation of a four-fenestrated physician-modified endograft using the Bolton TREO platform for complex abdominal aortic aneurysms.
CASE PRESENTATION
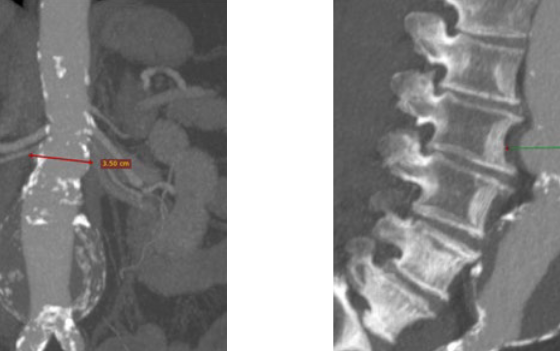
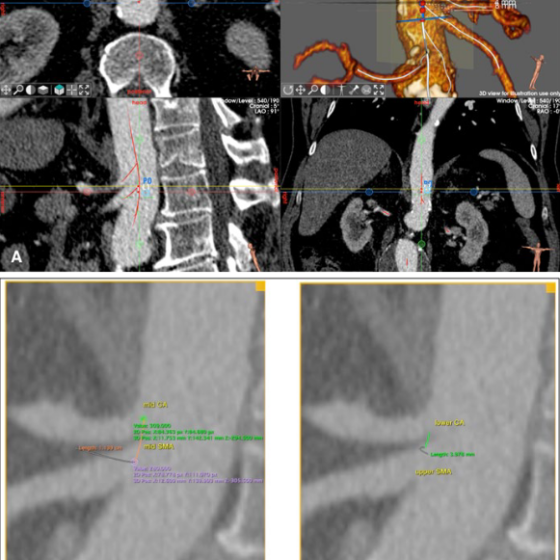
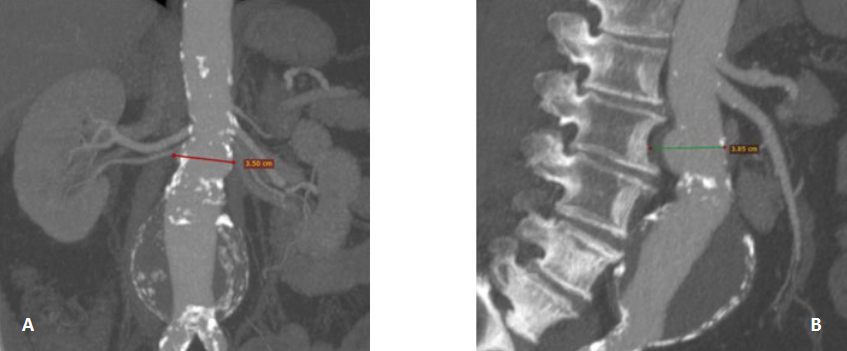
A 74-year-old obese male (BMI >31) presented to the emergency department with acute abdominal pain radiating to the back. His medical history was significant for arterial hypertension, dyslipidemia, chronic obstructive pulmonary disease, active smoking, and coronary artery disease. Three months prior, he had undergone coronary angioplasty for angina and was receiving dual antiplatelet therapy. Computed tomography angiography demonstrated a 7.2-cm juxtarenal abdominal aortic aneurysm, with an infrarenal neck diameter of 3.8 cm (Fig. 1A-B). Given the patient’s symptoms and significant comorbidities, an endovascular approach using a physician-modified endograft (PMEG) was selected.
HOW I DID IT
1. Preoperative Measurements and Planning on Computed Tomography Angiography
This technique is applied in patients with cAAA, including AAAs with a short proximal neck (<5mm), juxtarenal, pararenal, paravisceral aneurysms, as well as certain type IV thoracoabdominal aortic aneurysms. This is particularly appropriate for urgent or emergency situations, such as symptomatic aneurysms, in which CMDs are not readily available.
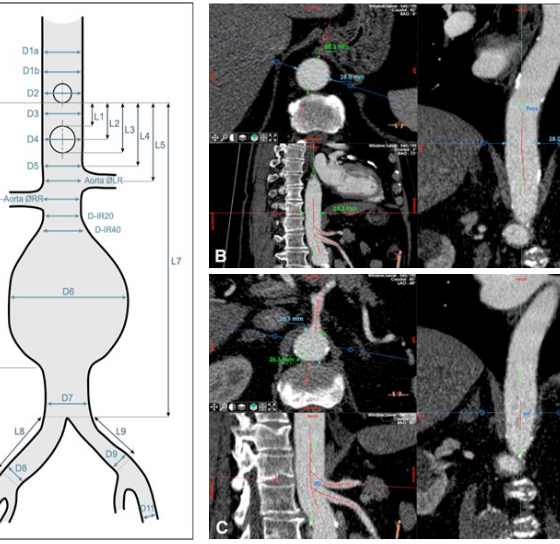
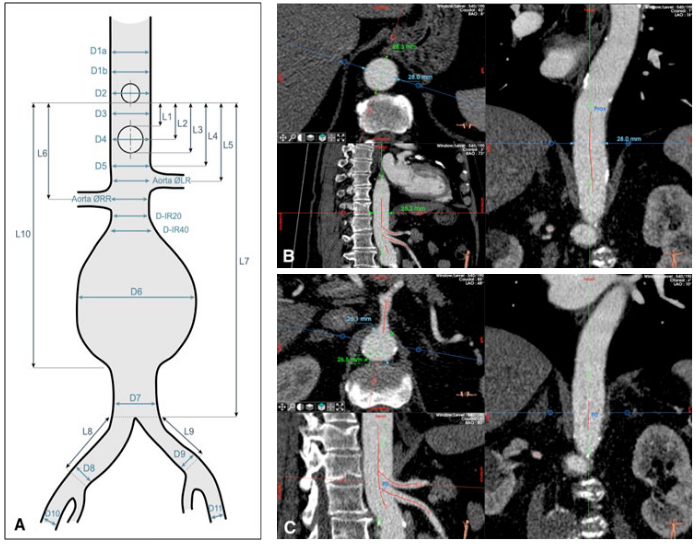
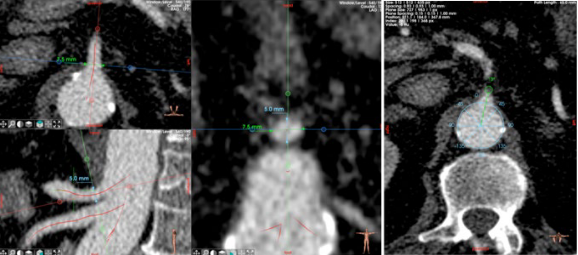
Preoperative planning was performed using high-resolution computed tomography angiography (CTA). All measurements were obtained and independently cross-checked using EndoSize and Horos to ensure accuracy and reproducibility. The aortic diameter was measured at the planned proximal sealing zone above the celiac trunk (CT), followed by systematic diameter evaluation along the entire length of the aorta down to the distal sealing zone. Simultaneously, longitudinal length measurements of the aorta were performed to determine the required graft length and the relative position of the visceral vessels (Fig. 2A-C).
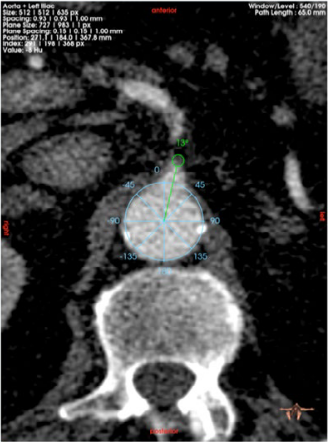
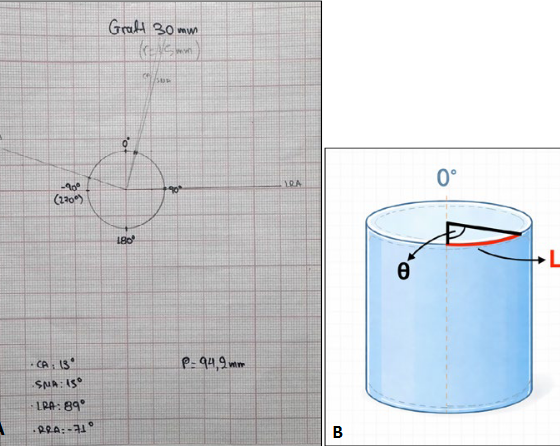
Taking into consideration the diameter and length measurements, the suitable TREO stent graft was selected, with careful consideration of both the main body diameter and length to ensure adequate proximal and distal sealing while accommodating the planned fenestrations. The circumferential orientation of each target vessel, including the celiac trunk (CT), the superior mesenteric artery (SMA), and the right and left renal arteries (RAs), was evaluated on axial CTA images. Clock positions were measured in degrees, using the 12:00 o’clock position as the reference point equivalent to 0°. The angular deviation of each target vessel’s ostium from the 0° point was calculated and defined as the θ (theta) angle. This angle was measured from the center of the aortic lumen to the center of the vessel ostium. Fig. 3 illustrates an example of how the θ angle was measured for the celiac trunk.
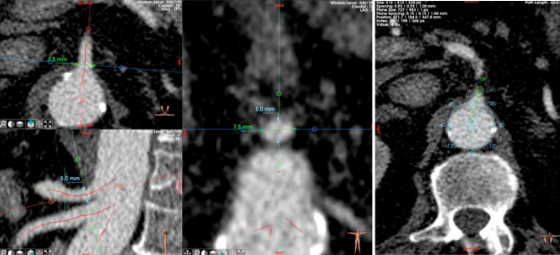
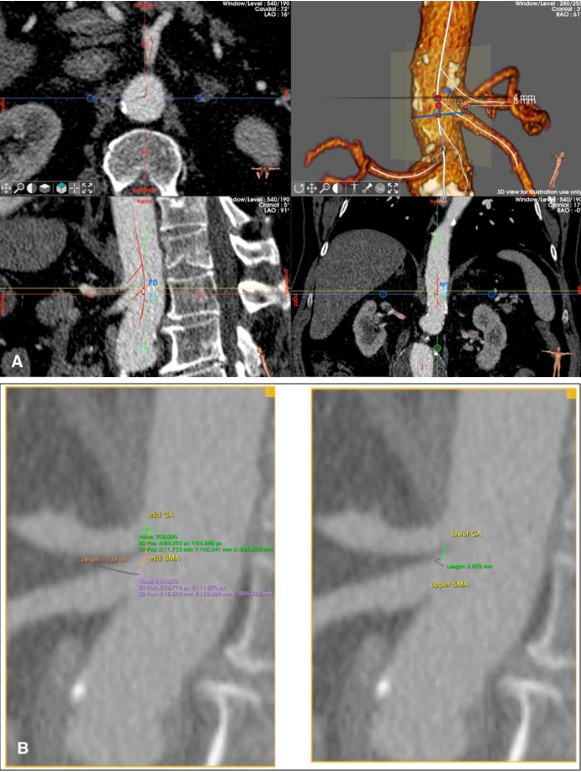
The diameters of each target vessel were assessed at both the ostial and distal landing segments. These measurements help determine the size of each fenestration, which is designed to be approximately 1 mm larger than the native vessel diameter to aid cannulation while maintaining a proper seal. Fig. 4 shows typical measurements of the diameters of the target vessels. Simultaneously, the landing length of each target vessel is evaluated to determine the required length for safe deployment and sealing of the bridging stent grafts.
Finally, the longitudinal distances between the visceral vessel ostia were meticulously measured. The primary measurements were obtained between the midpoint of the CT ostium and the midpoint of the SMA ostium (mid-CT to mid-SMA), as well as between the midpoint of the CT ostium and the midpoints of the right and left RA ostia (mid-CT to mid-RRA and mid-CT to mid-LRA). To enhance accuracy and provide internal verification, confirmatory measurements were taken from the lower margin of the CT ostium to the upper margin of each target vessel ostium, including the SMA, RRA, and LRA (lower CT to upper SMA, lower CT to upper RRA, and lower CT to upper LRA). These measurements were used to confirm longitudinal alignment and minimize cumulative errors during the positioning of the fenestrations (Fig. 5A-B).
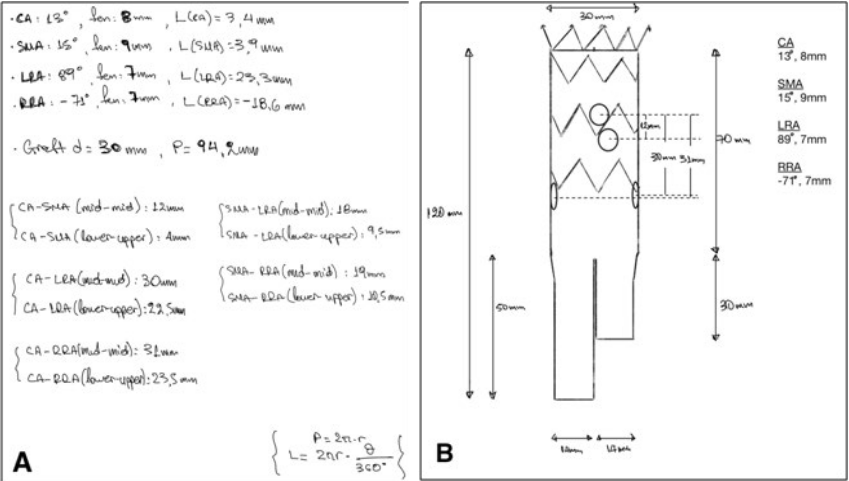
Graft Template Creation and Fenestration Mapping
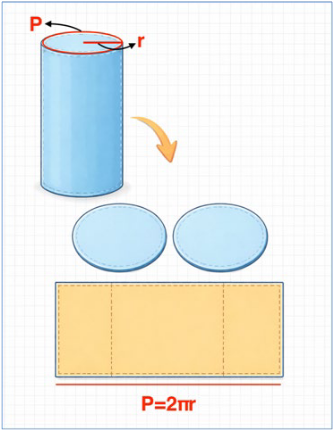
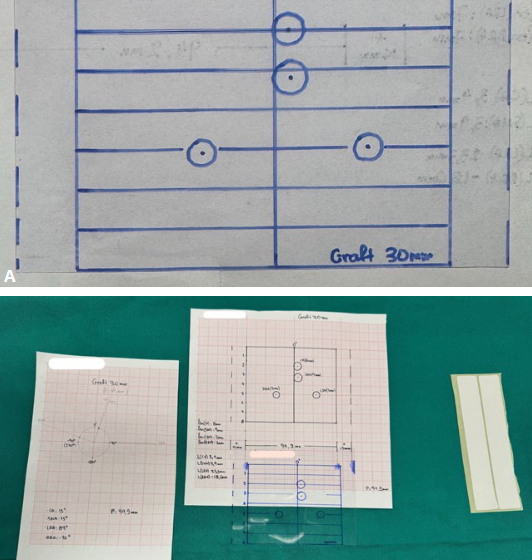
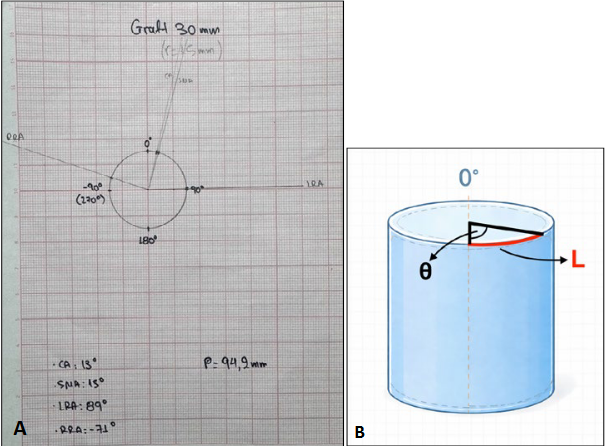
To convert preoperative CTA measurements into a consistent modification plan, the selected TREO graft was first recreated on millimeter paper using the development of a cylinder, which converted the three-dimensional graft shape into a two-dimensional template. The perimeter of the graft was calculated using its diameter using the formula P = 2πr, where r represents the graft radius. This perimeter represents the transverse width of the graft when it is unfolded. For example, for a graft with a 30-mm diameter (r= 15 mm), the calculated development is 94.2 mm (Fig. 6).
The circumferential position of each target vessel was determined based on the previously calculated θ angles, referenced from the 12 o’clock (0°) position.
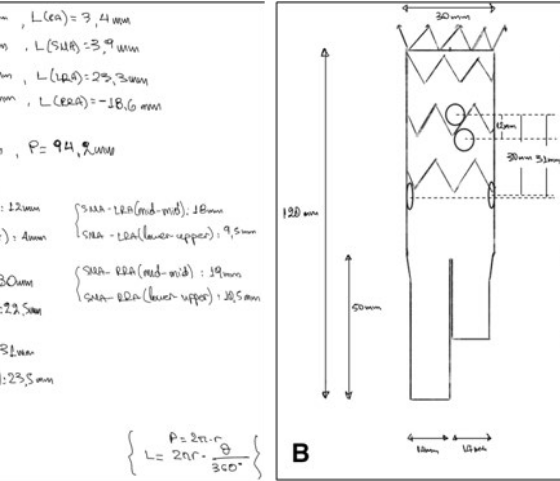
Each angular measurement was converted into a linear distance along the graft circumference, defined as the arc length (L), using the formula L = 2πrθ / 360. This conversion enables the precise placement of the clock positions derived from the CTA onto the two-dimensional graft template (Fig. 7A-B).
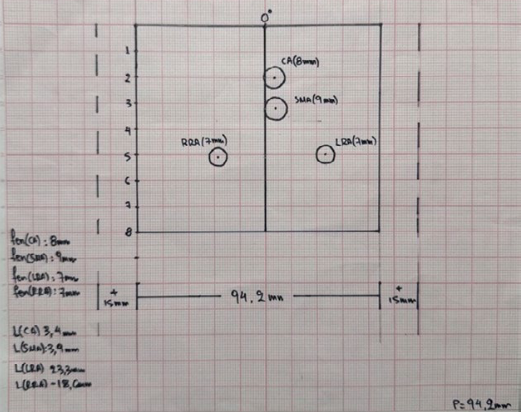
For instance, when the CT originates at an angle of 13°, the arc length for a 30 mm diameter graft is L(CT)=3.4 mm. This measurement represents the straight-line distance from the 12 o’clock reference line to the center of the CT fenestration on the unfolded graft template. To accurately place the CT fenestration, the 12 o’clock reference line is initially drawn on millimeter paper, followed by the calculated arc length and intended fenestration diameter. This process was repeated for the superior mesenteric, right, and left renal arteries.
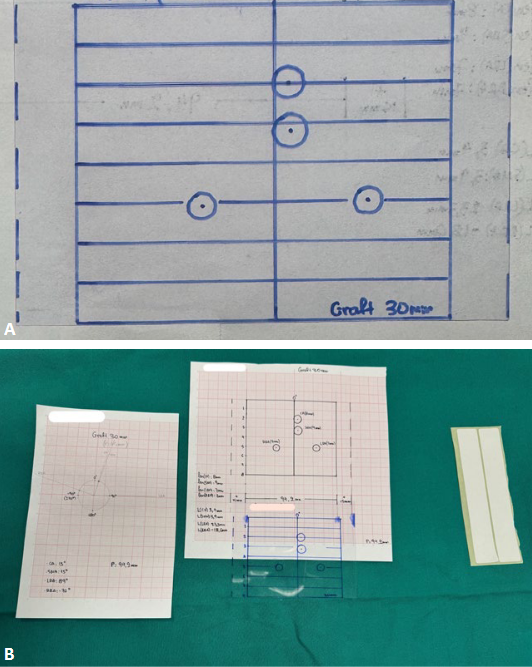
Based on the longitudinal distance measurements obtained from the CTA, the remaining visceral fenestrations were designed relative to the CT. The distances between the midpoint of the CT ostium and the midpoints of the superior mesenteric and renal arteries were mapped onto the template along the longitudinal axis, creating a complete patient-specific layout with four fenestrations. Fig. 8 displays the final version of the stent graft representation on millimeter paper.
Once the graft design is finalized, the template is transferred onto a clear, flexible plastic sheet, creating an exact duplicate of the millimeter-scale paper layout. All fenestration positions and dimensions are marked on this plastic sheet, which is later used as a patient-specific punch card during graft modification. The plastic punch card and the original millimeter paper template undergo plasma sterilization to ensure safe introduction into the sterile environment (Fig. 9A-B).
Based on all the above measurements and calculations, a schematic design of the stent graft was developed, showing the expected locations of the fenestrations, as illustrated in Fig. 10A-B.
2. Graft Deployment and Modification
Before modifying the graft, a dedicated sterile back table was set up in the operating room. The setup consisted of a sterilized clear plastic punch card, 5-0 and 6-0 monofilament polypropylene sutures (Prolene), nylon tapes, vessel loops, a rubber tube, a surgical cautery, a radiopaque marker, and 0.018-inch hydrophilic guidewires. All materials are organized to allow an uninterrupted workflow while maintaining strict, sterile conditions (Fig. 11).
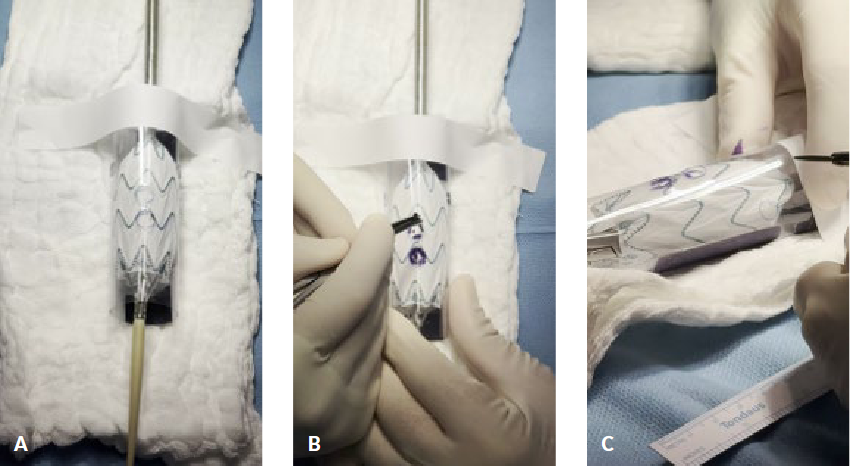
Before graft deployment, the stent graft was positioned under C-arm fluoroscopy to confirm the correct orientation of the device. Once the correct orientation was confirmed, the graft was partially deployed on the back table, with the deployment limited to the initial four stents, while ensuring that the contralateral limb remained undeployed. Partial deployment ensures that the graft fabric is adequately exposed for necessary modifications while preserving the ability to resheath the device (Fig. 12).
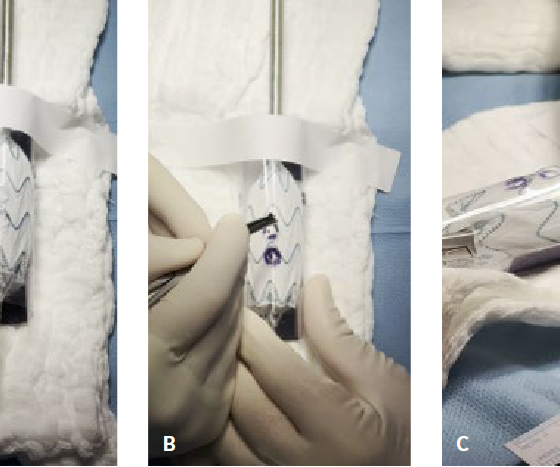
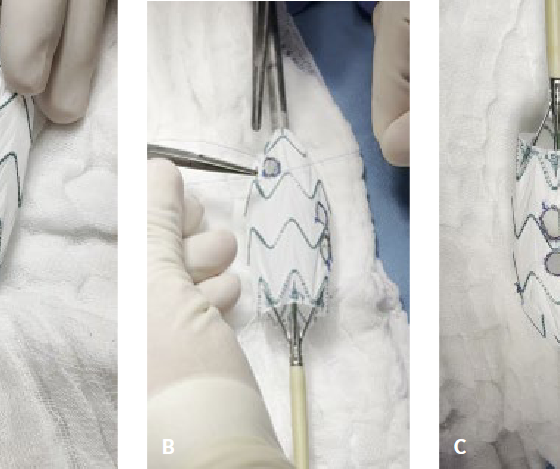
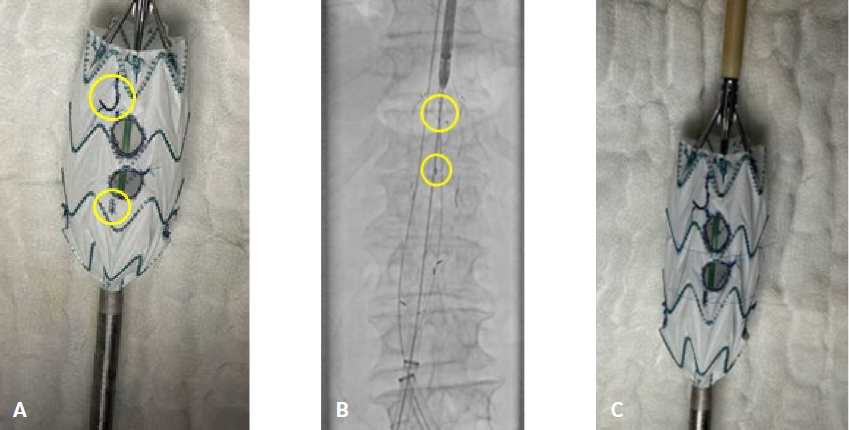
A tube was constructed from the punch card, and fenestrations were initially created in the clear plastic punch card at predetermined locations using surgical cautery. The punch card was then carefully placed over the partially deployed stent graft and precise alignment was verified. The 12 o’clock reference point and fenestration outlines were marked onto the graft fabric using a sterile marking pen (Fig. 13A-C).
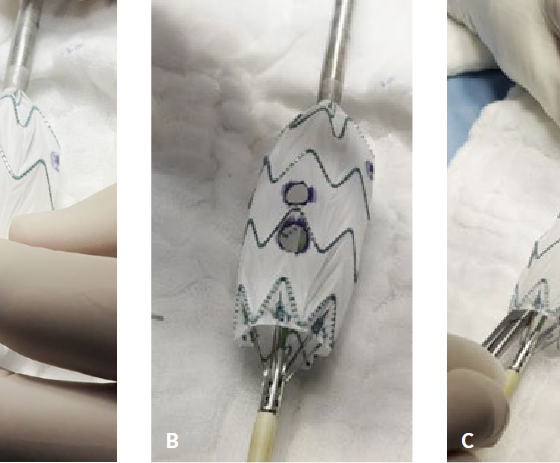
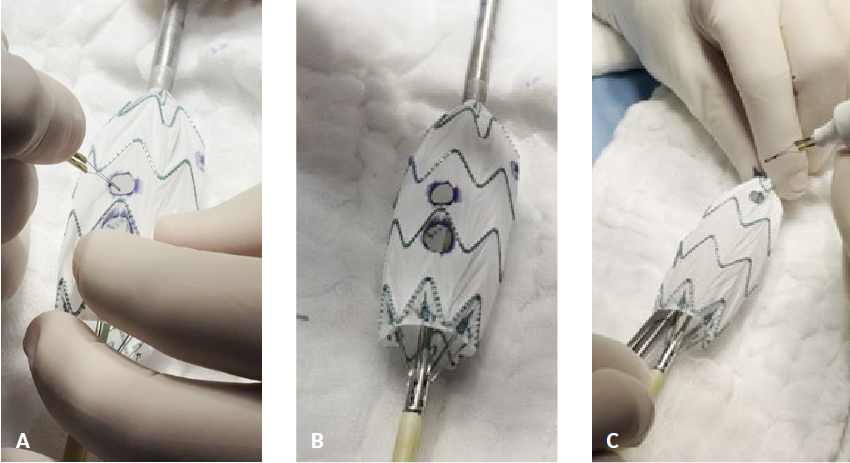
The punch card was subsequently removed, and the fenestrations were created directly on the graft fabric using the ophthalmic cautery, following the marked outlines as shown in Fig. 14A-C.
Each fenestration was then reinforced using the floppy tip of a 0.018-inch hydrophilic guidewire, which was shaped to fit the circumference of the fenestration. The guidewire was secured to the graft fabric with a continuous 5-0 monofilament polypropylene suture (Fig. 15A-C).
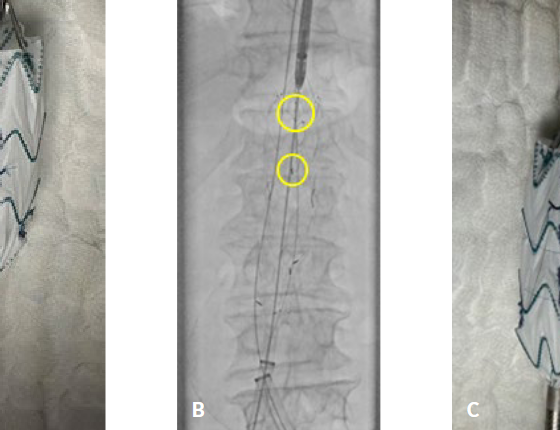
To achieve accurate graft alignment during implantation, two radiopaque markers were positioned at the 12 o’clock location. A J-shaped marker formed from the same guidewire used for fenestration reinforcement was placed proximally to the celiac trunk fenestration. In addition, a straight longitudinal marker provided by Terumo was placed immediately distal to the superior mesenteric artery fenestration.
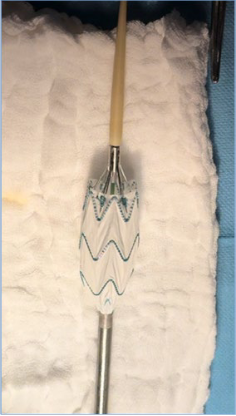
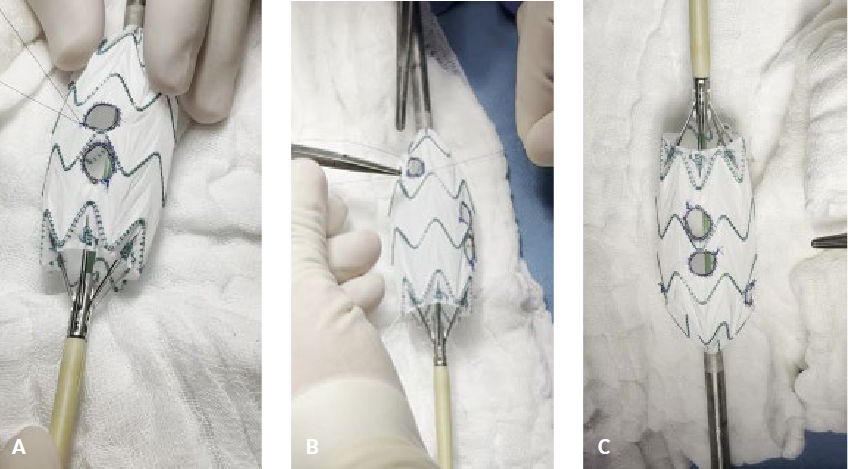
Finally, circular diameter-reducing ties are wrapped around the stent graft using a 6-0 monofilament polypropylene suture, achieving a reduction of approximately 40% in the graft diameter. This diameter-reduction ties aids in the controlled deployment and cannulation of the target vessels (Fig. 16A-C).
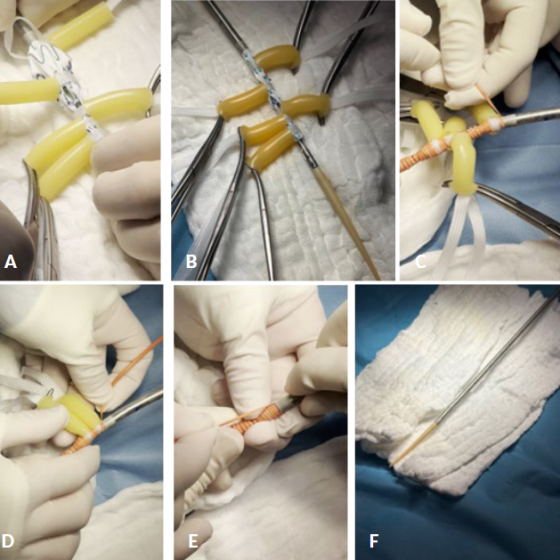
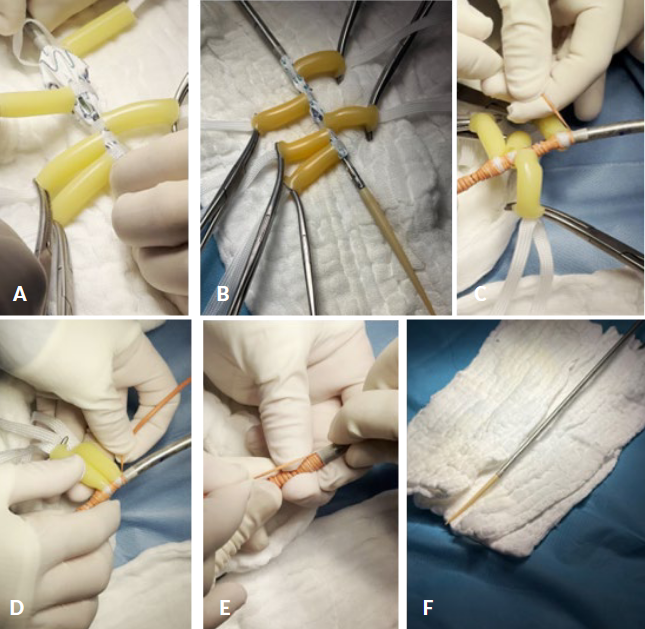
Following fenestration reinforcement, marker placement, and application of diameter-reducing ties, the graft was prepared for re-sheathing. Control of the deployed endograft was achieved using five nylon tapes passed through a rubber tube, which were wrapped around the deployed stent rings, and an additional tape was placed between the first and second stents, encircling the graft fabric. This configuration allowed control of the radial force of the stent rings, thereby preventing them from expanding during re-sheathing.
To further reduce excess graft fabric and ensure smooth reinsertion into the delivery sheath, vessel loops are applied longitudinally. One vessel loop was placed starting from the proximal end of the graft, while another was applied from the distal part, gradually reducing any excess fabric.
Once the radial force and fabric volume are adequately controlled, the graft is carefully re-sheathed, ensuring the preservation of fenestration alignment, reinforcement integrity, and marker orientation. During this phase, it is crucial to keep the 12 o’clock reference point stable and prevent any twisting or warping of the modified segment (Fig. 17A-F).
3. PMEG Implantation
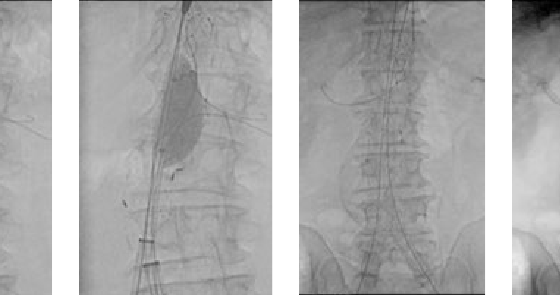
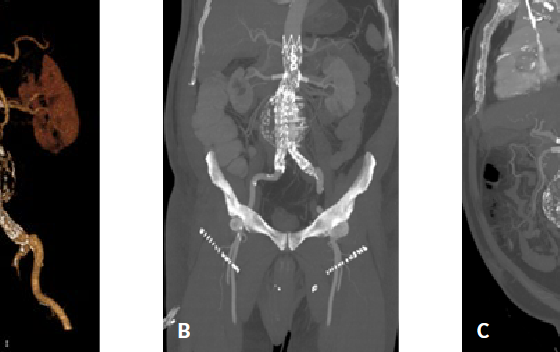
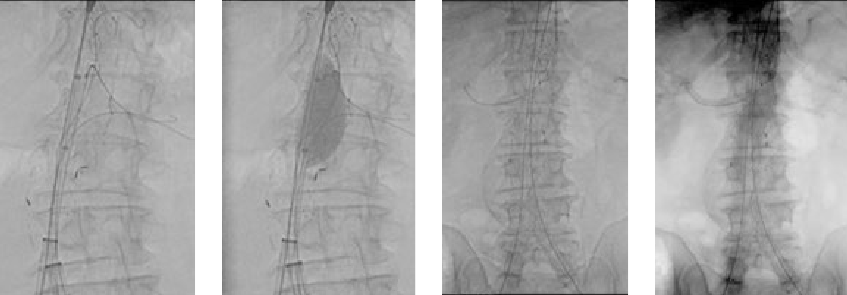
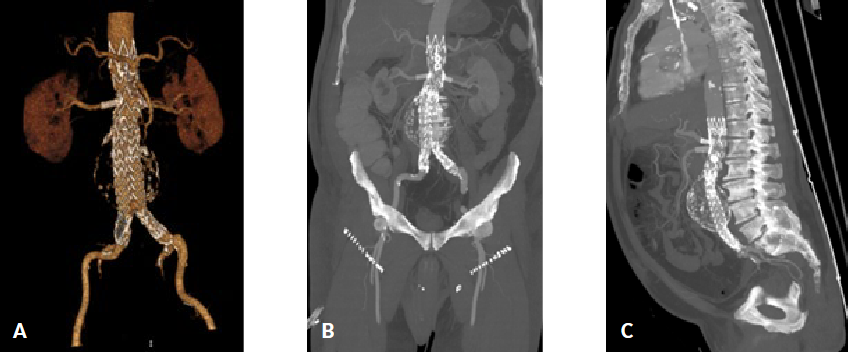
After bilateral surgical preparation of the common femoral arteries and systemic heparinization with 5.000 IU, the prepared device TREO (30-120) was introduced through a 20-F (33-cm) transfemoral sheath (DrySeal; Gore Medical, Flagstaff, AZ). After angiography and identification of the target vessels, orientation of the fenestrations followed and the device was gradually deployed up to the level of the contralateral gate. The contralateral limb was subsequently cannulated, and a 22-F (33-cm) transfemoral sheath (DrySeal; Gore Medical) was inserted. Target vessel cannulation was performed via a retrograde (CA, SMA and left renal from below) and antergrade (right renal from axillary artery) approach using a 7-Fr sheath. A steerable introducer (Fustar; Lifetech Scientific; tip deflection 0°-160°) was utilized to facilitate selective catheterization of the target vessels. A 260-cm Rosen wire (Cook Medical Inc., Bloomington, IN) was advanced and positioned within each target artery, after which the main body of the endograft was fully deployed. The diameter-reducing ties were subsequently released using a 46-mm compliant balloon (Coda; Cook Medical Inc.). Subsequently, balloon-expandable covered stents were sequentially deployed and flared within the target vessels: the celiac artery (BeFlared Bentley, 8/10-27 mm), the superior mesenteric artery (Advanta V12, Getinge 9-32 mm), the left renal artery (Advanta V12 7-22 mm), and the right renal artery (Advanta V12, 7-32 mm). This was followed by deployment of the bilateral iliac limbs [left 20-140 mm, right 24-140 mm, (Figure18A-C)]. Final anteroposterior and lateral completion angiography confirmed the absence of endoleak. The patient was extubated, a neurological examination was performed, and the patient was transferred to the vascular surgery ward. A predischarge computed tomography angiography was obtained and confirmed appropriate device configuration and the absence of endoleak (Figure19A-C). The patient was discharged with dual antiplatelet therapy and follow-up was scheduled according to the standard FEVAR surveillance protocol.
CONCLUSION
Physician-modified endografts provide a valuable and versatile solution for treating complex abdominal aortic aneurysms in settings where custom-made devices are unavailable or when time limitations prevent their use. The technique described outlines a systematic, reproducible method for creating a four-fenestrated physician-modified endograft using the Bolton TREO platform, with emphasis on meticulous preoperative planning, precise fenestration mapping, controlled graft modification, and secure re-sheathing.
This method seeks to improve the precision, consistency, and orientation during surgery by converting 3D imaging data into a uniform 2D graft template and applying a punch card technique. When conducted at specialized centers and applied to appropriately selected patients, this technique enables the safe execution of complex aneurysm repair using established FEVAR implantation principles. Continued experience, careful management, and long-term follow-up are crucial to further establish durability and optimize outcomes.
REFERENCES
- Wanhainen A, Van Herzeele I, Bastos Goncalves F, Bellmunt Montoya S, Berard X, Boyle JR, et Editor’s Choice -European Society for Vascular Surgery (ESVS) 2024 Clinical Practice Guidelines on the Management of Abdominal Aorto-Iliac Artery Aneurysms. Eur J Vasc Endovasc Surg. 2024;67(2):192-331.
- Raulli SJ, Gomes VC, Parodi FE, Vasan P, Sun D, Marston WA, et al. Five-year outcomes of fenestrated and branched endovascular repair of complex aortic aneurysms based on aneurysm Journal of Vascular Surgery. 2024 1;80(2):302-10.
- Oderich GS, Tenorio ER, Mendes BC, Lima GBB, Marcondes GB, Saqib N, et al. Midterm Outcomes of a Prospective, Nonrandomized Study to Evaluate Endovascular Repair of Complex Aortic Aneurysms Using Fenestrated-Branched Endografts. Ann Surg. 2021;274(3):491-9.
- Çekmecelioglu D, Orozco-Sevilla V, Coselli JS. Open vs. endovascular thoracoabdominal aortic aneurysm repair: tale of the tape. Asian Cardiovasc Thorac Ann. 2021;29(7):643-53.
- Oderich GS, Ricotta Modified Fenestrated Stent Grafts: Device Design, Modifications, Implantation, and Current Applications. Perspectives in Vascular Surgery and Endovascular Therapy. 2009;21(3):157-67.
- Gouveia E Melo R, Fernández Prendes C, Caldeira D, Stana J, Rantner B, Wanhainen A, et al. Systematic Review and Meta-analysis of Physician Modified Endografts for Treatment of Thoraco-Abdominal and Complex Abdominal Aortic Aneurysms. Eur J Vasc Endovasc Surg. 2022;64(23):188-99.
- Tsilimparis N, Gouveia E Melo R, Tenorio ER, Scali S, Mendes B, Han S, et al. Multicenter Study on Physician-Modified Endografts for Thoracoabdominal and Complex Abdominal Aortic Aneurysm Circulation. 2024;150(17):1327-42.
- Chait J, Tenorio ER, Hofer JM, DeMartino RR, Oderich GS, Mendes BC. Five-year outcomes of physician-modified endografts for repair of complex abdominal and thoracoabdominal aortic J Vasc Surg. 2023;77(2):374385.e4.
- Robaldo A, Ruffino MA, Garbero E, Amrein E, Giovannacci L, Giorno RD, et al. Indications, planning, and technical aspects in physician-modified endografts based on a cross-sectional global survey. J Vasc Surg. 2025;82(3):760769.e9.
- Piazza M, Spertino A, Colacchio EC, Volpe A, Pratesi G, Trimarchi S, et al. Early Outcomes from the Multicentre Standardised PHysician Modified Four Fenestration Endograft REgistry (S.PH.E.RE.). Eur J Vasc Endovasc Surg. 2025;70(6):735-43.
- Ducasse E, Berard X, Caradu C. Physician modification of the Terumo Aortic TREO device for juxtarenal or pararenal aortic aneurysms. Journal of Vascular Surgery Cases, Innovations and Techniques. 2024;10(3):101458.
- Lescan M, Dimov A, Turchino D, Toma A, Scheumann J, Berger T, et al. Suitability of Endovascular Materials for Physician-Modified Fenestrated Endografts in Urgent Juxtarenal and Pararenal Aortic Pathologies. J Clin Med. 2025;14(14):4830.
- Hüttl A, Szentiványi A, Bérczi Á, Juhos B, Szablics FÉ, Osztrogonácz P, et Using a Standard Infrarenal Bifurcated Device as a Quadruple-Fenestrated Physician-Modified Endograft for Complex Abdominal Aortic Aneurysms-A Simulation Study. JCM. 2025;14(12):4249.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}