The role of Oncovascular Surgery in Primary Retroperitoneal Sarcomas

| Available Online: | October, 2025 |
| Page: | 137–143 |
Author for correspondence:
Melina Stathopoulou, MD
Department of Surgery, General University Hospital of
Patras, Patras Medical School, Patras, Greece E-mail: melinastath@gmail.com
doi: 10.59037/7ryg6973
ISSN 2732-7175 / 2025 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications All rights reserved. https://www.heljves.com
Melina Stathopoulou1, Spyros Papadoulas2, Eleanna Serraou1, George Theofanis1, Despoina Zampetaki1, Chrysanthi Papageorgopoulpou2, Petros Zampakis3, Francesk Mulita4, Ioannis Maroulis1
1 Department of Surgery, General University Hospital of Patras, Patras Medical School, Patras, Greece
2 Department of Vascular Surgery, General University Hospital of Patras, Patras Medical School, Patras
3 Department of Radiology, General University Hospital of Patras, Patras Medical School, Patras, Greece
4 Department of Surgery, General Hospital of Aigion, Greece
Full Text
Gallery
Full Text
Abstract:
Retroperitoneal soft tissue sarcomas are a rare clinical entity, with an annual incidence of less than 0,5 in 100.000. Sur- gical resection is the main therapeutic option for patient with favourable characteristics, with radiotherapy and neoad- juvant chemotherapy being utilised pre-operatively to optimise the tumour characteristics and are not often employed as stand-alone treatment. R0 resection is the most essential factor for achieving a long-term recurrence-free survival. Due to their close anatomic relations and their infiltrative character towards the abdominal vessels, en bloc resection of these tumors often requires a complex vascular reconstruction. Lack of standardised techniques or guidelines only adds to the complexity. After review of the recent literature, we summarize important information about the pathogenesis, diagnosis and treatment of retroperitoneal soft tissue sarcomas. We additionally analyse strategies employed by onco- vascular surgeons that both preserve the vascular supply to the intraabdominal organs and lower extremities, after en block resection of the tumour along with infiltrated vessels. These include vessel ligation, or repair after partial or total resection. These strategies aid in the achievement of an optimal oncological outcome.
INTRODUCTION
Retroperitoneal soft tissue sarcomas (RSTSs) are rare malignant tumours arising from mesenchymal cells. RSTS account for 15% of all soft tissue sarcomas, with those affecting the extremities being most common. RSTSs are characterized by large variability in histologic type, with liposarcomas being the most prominent subtype, making up 1% of all malignant cancers in the adult population, followed by leiomyosarcomas1,2. According to the fifth edition of the WHO Classification of Tumours of Soft Tissue and Bone, the histological subtypes of liposarcomas include the atypical lipomatous tumour (ALT), also known as well-differentiated liposarcoma (WDLPS), dedifferentiated liposarcomas (DDLPS), myxoid liposarcomas (MLPS), pleomorphic liposarcomas (PLPS), and myxoid pleomorphic liposarcomas3, with each subtype having its distinct diagnostic and biologic features. Mean patient age at diagnosis ranges between 59-61 years4 and can either be an incidental finding or have symptoms due to extrinsic compression to other structures. Surgical resection is the only option offering the possibility of cure and recurrence-free survival. However, there seems to be distinct lack of official recommendations regarding the surgical management of retroperitoneal tumours involving the intraabdominal vessels, partly due to their heterogeneity, and partly due to vascular infiltration, which has been a criterion of non-resectability.
We performed a review study encountering the PubMed medical Database. The search strategy incorporated the following keywords: “primary retroperitoneal sarcomas”, “retroperitoneal sarcomas”, “oncovascular” ,“arterial”, “venous”, “vascular”, “reconstruction”, “repair” and combinations of them. Retrieved records were subsequently screened for relevance to the topic of the study. Cross reference was carried out to retrieve relevant studies. Our literature review (summarized in the Table) underscores the rarity yet clinical significance of retroperitoneal sarcomas resections along with the infiltrated vessels and combined with vascular reconstructions. We retrieved 9 case reports and 1 case series, including a total of 17 patients.
PATHOGENESIS
Mesenchymal tumours account for about 50% of all primary retroperitoneal tumours5. Due to their anatomical position, RSTSs often have no accompanying symptoms, thus remaining undetected and having grown to considerable size when diagnosed. In cases of sarcomas with large diameters, an increase in abdominal circumference and a palpable mass can be the first signs of RSTS. Other symptomatology can affect the digestive tract, the urinary tract (renal impairment, ureter obstruction due to extrinsic compression or infiltration), the vascular network (extrinsic compression, infiltration or malignant thrombus formation leading to phlebitis, edema secondary to partial or total occlusion), as well as nerve compression6,7.
Another consideration is the tendency to arise in narrow proximity to vascular structures, making RSTSs historically Table. Demographic, surgical and follow-up data of 17 patients with retroperitoneal sarcomas, who underwent resection and simultaneous vascular reconstruction
| Date of
Publication |
Authors Age, gender | Histological identity, involved structures | Pre-operative
treatments |
Resection plan |
Reconstruction
strategy |
Recovery |
| April 2025 | Kotsis et 63yo | Myxofibrosarcoma | Pre-op | R0 resection (En | IVC replacement with | |
| al. [24] (M) | involving the IVC | radioRX and | bloc resection | PTFE tube graft | ||
| chemotherapy | of the sarcoma, | |||||
| (doxorubicin | the IVC, the right | |||||
| ifosfamide) | kidney and psoas- | |||||
| à partial | quadriceps muscle | |||||
| radiographic | portions) | |||||
| response | ||||||
| Jan 2024 | Bael et al. 42yo | Leiomyosarcoma | R0 resection with | IVC reconstruction | Old hematoma | |
| [30] (F) | involving the IVC | nephrectomy | with a Dacron graft | drainage on 3rd | ||
| in close proximity | post-op week. RT | |||||
| with the left | from 4th post-op | |||||
| kidney | month on | |||||
| Jul 2023 | Castro et 48yo
al. [31] (F) |
Well-differentiated
liposarcoma |
En bloc resection, along with the entire retrohepatic IVC | No reconstruction | Freer of disease, attending followups | |
| Dec 2021 | Hasega 72yo | Soft tissue high- | Radical tumour | Saphenous vein | Local recurrence | |
| wa et al. [22] (M) | grade sarcoma | resection | graft to reconstruct | at patch site | ||
| occluding the | after SMA | the SMA, aortic | on 6th post-op | |||
| celiac trunk and | reconstruction | defect reconstructed | month. Received | |||
| the origin of the | with Dacron patch, | chemotherapy, | ||||
| SMA | arterial bypass for | patient alive w/o | ||||
| the common hepatic | recurrence at 6th | |||||
| artery with ringed PTFE | post-op year | |||||
| graft (intraoperatively | ||||||
| without pulse) | ||||||
| Nov 2021 | Tirnavean 74yo | Leiomyosarcoma | En bloc resection | Reconstruction of the | 2 years of | |
| et al. [32] | arising in the IVC | IVC with autologous | recurrence-free | |||
| near the renal | graft harvested from | survival | ||||
| ostia | the right superficial | |||||
| femoral vein | ||||||
| March 2021 | Kontopodis 62yo | Locally recurrent | Resection with | reconstruction with a | No post-op | |
| N et al. [35] (M) | myxoid | removal of both | bifurcated Dacron graft | complication, | ||
| liposarcoma | CIVs and infrarenal | patient discharged | ||||
| involving the CIV | IVC | on 11th post-op | ||||
| common iliac vein | day | |||||
| and distal IVC | ||||||
| Nov 2020 | Quildrian 54yo | Low-grade | En-bloc resection | Reconstruction with | Urgent | |
| et al. [29] (F) | sarcoma with | with resection of | bi-iliac PTFE graft | thrombectomy | ||
| infrarenal aorta | left psoas muscle, | and re- | ||||
| involvement | left nephrectomy, | anastomosis on | ||||
| partial aorta | post-op day 0, | |||||
| resection | patient alive and | |||||
| w/o recurrence 2 | ||||||
| years post-op | ||||||
| Aug 2020 | Grieff et 63yo | Leiomyosarcoma | Neoadjuvant | En-bloc resection | Combined aortocaval | 1 year recurrence- |
| al. [27] (M) | chemotherapy | of aorta, IVC, | reconstruction with | free survival | ||
| with | tumour and right | Dacron Gelsoft tube | ||||
| doxorubicin | kidney | graft for the aorta | ||||
| and | and temporary veno- | |||||
| dacarbazine | venous (femoral vein | |||||
| to internal jugular) | ||||||
| bypass, followed | ||||||
| by a ringed GORE | ||||||
| tex graft for the IVC | ||||||
| reconstruction |
| 2020 Homsy et 57yo Leiomyosarcoma No Marginal resection Reconstruction IVC thrombosis at
al.[7] (F) with resection of aorta with 33 months |
||||||
| of the infrarenal | polyethylene | |||||
| aorta and IVC | prosthesis, IVC with | |||||
| bovine pericardium | ||||||
| patch and temporary | ||||||
| axillobirenal bypass | ||||||
| 62yo | Metastatic | Marginal resection | Reconstruction | IVC compressed by | ||
| (F) | Leiomyosarcoma | with resection of | of the aorta with | recurrent tumour | ||
| without vascular | aorta, IVC and left | polyethylene Y graft, | at 13 months | |||
| invasion | renal vein, as well | IVC and left renal vein | and eventually | |||
| as resection of the | with homograft vein | patient died to the | ||||
| right kidney | neoplasm at post- | |||||
| operative month | ||||||
| 15 | ||||||
| 56yo | Leiomyosarcoma | Pre-operative | Marginal resection | Reconstruction of | Thrombectomy | |
| (F) | embolization of | with resection of | the left iliac vein with | and stent at post- | ||
| tumor-feeding | the left iliac vein, | autologous vein graft | op day 5, patient | |||
| arteries | sigmoid colon, and | died at post-op | ||||
| left nephrectomy | month 22 | |||||
| 26yo
(M) |
Leiomyosarcoma
, involving the |
Marginal resection
of tumour with |
Reconstruction with
polyethylene |
Disease-free at 25th month post- | ||
| aorta, SMA, | pancreatectomy, | op | ||||
| hepatic artery and | splenectomy and | |||||
| right renal artery | left nephrectomy | |||||
| 58yo | Leiomyosarcoma | Marginal resection | Homograft vein | Disease-free at 6th | ||
| (F) | involving the IVC | of tumour | reconstruction | post-op year | ||
| 61yo
(F) |
Leiomyosarcoma
involving the IVC |
Wide resection of
tumour and right |
IVC reconstruction with homograft vein | Living with sarcoma at 6th | ||
| and left renal vein | nephrectomy | and renal vein with | post-op year | |||
| autologous vein graft | ||||||
| 59yo | Sclerosing | Marginal resection | Reconstruction using | Local recurrent | ||
| (F) | liposarcoma | of tumour with | homograft vein | tumour | ||
| involving the IIA, | hysterectomy | compressing the | ||||
| EIA, IIV, EIV | IVC at 4 months. | |||||
| Dead 1 year after | ||||||
| her operation | ||||||
| 32yo | Angiosarcoma | Resection with | Reconstruction of | Disease-free 2 | ||
| (M) | epithelioeides | right nephrectomy | the aorta, SMA, | years after | ||
| arising from the | celiac trunk, left | |||||
| aorta, involving | renal vein and both | |||||
| the IVC and the | internal iliac arteries | |||||
| celiac trunk | with polyethylene | |||||
| prosthesis, IVC with | ||||||
| bovine pericardium. | ||||||
| Additionally temporary | ||||||
| axillo-renal bypass | ||||||
| May 2020 Yokohama | 59yo | Dedifferentiated | Neoadjuvant | Resection with | Femoro-femoral | Patient free of |
| et al.[11] | (F) | liposarcoma | chemotherapy | right common iliac | bypass | recurrence at 1 |
| with | artery and vein | year post-op | ||||
| doxorubicin | resection, right | |||||
| and ifosfamide. | nephrectomy, and | |||||
| Femoro- | resection of right | |||||
| femoral arterial | psoas muscle and | |||||
| bypass before | femoral nerve | |||||
| laparotomy | ||||||
Abbreviations: M: Male, F: Female, EIA: external iliac artery, EIV: external iliac vein, IIA: internal iliac artery, IIV: internal iliac vein, IVC: inferior vena cava, pre-op: preoperative, post-op: post-operative, PTFE: polytetrafluoroethylene, RT: radiotherapy, SMA: superior mesenteric artery, yo: years old.
Challenging to resect. A R0 excision requires wide dissection and removal of portions from the surrounding organs or muscles, and that often includes the large intra-abdominal vessels. Additionally, local recurrence is more frequent in patients who have undergone surgical resection of a primary RSTP compared to patients with extremity STS8. Thus, the need for wide resection while simmultaneusly keeping the vascular integrity of the abdominal organs has made the vascular surgeon an integral part of the multidisciplinary team for RSTS patients, giving rise to the field of oncovascular surgery.
DIAGNOSIS
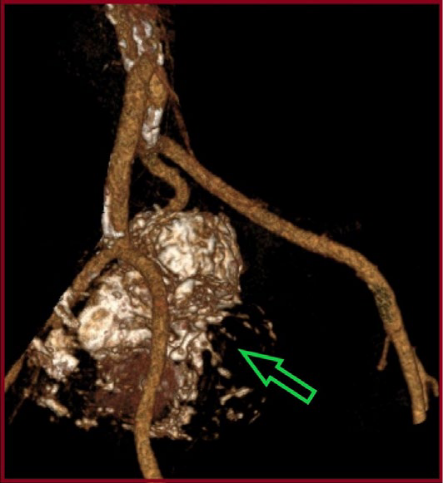
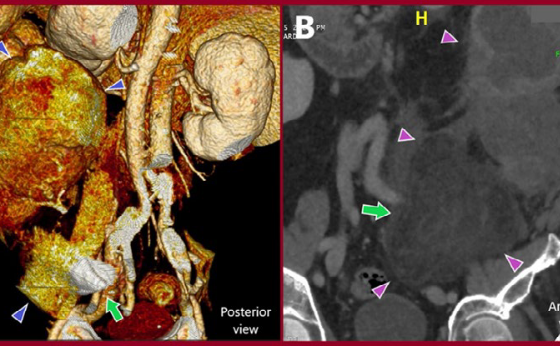
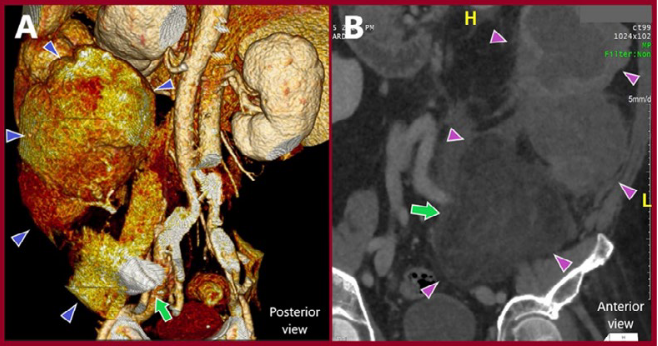
As stated earlier, RSTSs can be found incidentally during imaging for other complaints, otherwise they can grow into a large size before being diagnosed. Experts agree that computational tomography (CT) is the gold standard for the diagnosis of RSTSs (Figure 1,2). This is especially true for tumours invading the Inferior Vena Cava (IVC)9. Magnetic resonance imaging (MRI) can be supplementary and is thought to better detect vessel wall invasion. Due to the infiltrative nature of RSTSs, some researchers mention the MRI tail sign as a guide for planning the anatomical margins of resection10. Additionally, Magnetic Resonance Venography (MRV) can differentiate between ordinary or malignant thrombi and assist in mapping the extent of intraluminal thrombus, aiming to ultimately limit the intraoperative tumour dissemination, discussed later8,9.
As with every oncologic surgery, a pre-operative biopsy should always be available, since a variety of tumours other than sarcomas can result in a retroperitoneal mass and which are optimally managed with modalities other than resection. A biopsy can only be omitted only in the rare case of a WDLPS or DDLPS8.9. For tumors invading the IVC, a CT-guided core needle biopsy should be preferred9. An MRI-guided biopsy can be obtained from the least well-differentiated area of the tumor, using specific advanced protocols8. A retroperitoneal approach is usually preferred to limit tumor dissemination and avoid damage to endoperitoneal organs. An open or minimally invasive surgical biopsy should be avoided for the same reason8.
TREATMENT
A multidisciplinary team should summarize imaging and pathology results, as well as patient parameters and discuss the treatment plan. Neoadjuvant chemotherapy and radiotherapy (RT) are recommended for intermediate and high-grade lesions to mitigate the risk of local and distant recurrence and improve surgical outcomes. Recent guidelines advise for use of neoadjuvant systemic therapy in cases high risk for metastases or as a means of downstaging to allow resection11. However, it is not recommended for low-grade RSTSs and results are generally not hopeful12, 13-17. Radiotherapy has been shown to aid the control of local recurrence in patients undergoing en bloc resection with wide margins, but not in the overall survival of these patients. There is a tendency to extend overall survival but without conclusive results12,18, 19. Thus, neoadjuvant RT should be employed in patients with a high risk of local recurrence and should not be considered as a standard in the treatment in RSTS patients. RT toxicity is an additional factor that should be taken into account. Ultimately, the decision for administration of neoadjuvant therapy is made by the oncologist, depending on the performance status of the patient.
There are different strategies depending on the vascular and non-vascular structures involved when planning the surgical resection of RSTSs. Conversely, the involvement of the celiac trunk, the superior mesenteric artery, portal vein, invasive extension into the right atrium and infiltration of multiple organs such as pancreas and liver are criteria of non-resectability20. Nonetheless, recent advances in technology and technical skills have allowed progress to be made regarding tumour infiltrating the large intraabdominal vessels up to the level of the juxtarenal aorta.
Surgical therapy has two distinct goals: the first is to resect the tumour with a wide margin, macroscopically free of infiltrations, and the second is to minimize blood loss and avoid circulatory compromise. In cases of inferior vena cava (IVC) infiltration, IVC ligation can be considered in tumours lower than the renal ostia or tumours causing external obstruction of the IVC, providing that adequate collateral circulation has been established9. If less than 50% of the lumen is obstructed, or in the case that the suprarenal IVC is involved, then the IVC should be repaired. Repair by primary suture is not realisable, since the tumours often encase the IVC in a considerable length, also considering the need for a wide resection margin, creating distance between the two ends. There is also the possibility of partial vascular resection, with such an approach mainly utilised for veins due to their compliance. In this case, repair of venotomy can be achieved by primary suture, a biologic or a synthetic patch21.
In cases of primary sarcomas of the aorta or of DDLPSs involving the infrarenal aorta, the involved segment is excised and replaced by a synthetic graft. If the juxtaor supra-renal aorta is involved, the complexity of repair increases due to the need to reimplant the renal arteries, the superior mesenteric artery, and the celiac trunk21,22. Homsy et al.7 report several cases of aortic resection in which reconstruction was successful and who succumbed to causes other than graft failure, proving that, despite the high-risk of complications, the benefit from an R0 resection should be weighed against it 23.
When it comes to graft repair, polytetrafluoroethylene (PTFE) grafts are the first choice. Autologous grafts can be utilized when infection is a concern, such when interventions on the intestines are needed7. However, they are being abandoned as they seem to compromise the oncological outcome24. Ringed PTFE grafts of smaller diameter than the original IVC seem to yield the best results, offering more support and resisting collapse to extrinsic pressure, thus maintaining adequate flow. This also lowers the risk of in-graft thrombosis, as graft flow is increased25,24,26.
Regarding in-graft flow and thrombus formation, there are several tools that several surgeons have used intraoperatively. The use of intraoperative doppler can confirm that in-graft flow is sufficient24. Likewise, transesophageal echocardiography (TEE) is used intraoperatively when it is suspected that an existing malignant thrombus extends to the supradiaphragmatic IVC9. Some authors have used an IVC filter to avoid pulmonary embolism due to malignant emboli or the creation of an arteriovenous fistula after IVC resection6. However, others do not recommend such practice, supporting that careful dissection of the IVC and good proximal and distal control are sufficient9. This requires mapping of thrombus extent, achieved via pre-operative MRI, intraoperative ultrasound and if necessary, TEE.
For tumors invading or surrounding the common, internal and/or external iliac arteries (CIAs, IIAs, EIAs respectively), often both arterial and venous reconstruction is required, owing to their close proximity27. The IIA can be ligated without limb compromise, while the CIA and EIA can be reconstructed with synthetic or biologic grafts28,21,29,30,31,32,23. In case of concomitant bowel resection, an extra-anatomical bypass might be considered21. The contralateral femoral artery or vein can be utilized as an autologous graft should biologic grafts be unavailable28,21. Should the graft pass over the inguinal ligament, a muscle flap can be constructed to protect it33 Similar to the IVC, the iliac veins can be reconstructed by biologic or PTFE graft or by an autologous contralateral femoral vein graft. Contrary to the IVC, smaller diameters yield a lower flow, thus lowering patency rates. Contralateral IIA transposition for reconstruction of the CIA is also described in patients with microscopic tumour infiltration34. Common and internal iliac veins can be safely resected, when infiltrated, accounting for the adequate collateral vessels draining the extremity. In any strategy it is important to avoid external compression of the grafts. Kontopodis N et al. 35 used a bifurcated graft to reconstruct the right common iliac vein, passing the left limb over the native right common iliac artery to avoid exactly that.
As extended resection of multiple organs is required to achieve R0 resection, timing of each one is crucial to the outcome. Kotsis et al. opted to first tackle the repair of the IVC and then followed the oncological resection of the tumour24. Although this logic allows for an ideal field for the tumour excision, it is not completely without risk of graft compromise.
Anticoagulation therapy is lifelong in the cases of graft repair. There are no established guidelines or a clear consensus. Pneumatic compression devices as well as prompt anticoagulation therapy in the immediate post-operative period is the optimal combination. There is the benefit of improving the flow rate in the reconstructed IVC by improving venous return24. Post-operative follow-up should include routine CT-angiography, starting in the 1st postoperative month to assess in-graft flow and thrombus formation, with the possibility to titrate the anticoagulation therapy further9. Upon unifocal recurrence, reintervention with complete excision is warranted, whereas in multifocal recurrence intervention is unlikely to be radical and has palliative character37.
CONCLUSION
RSTSs pose a complex challenge to the oncologic surgeon, often requiring extended vascular resections and replacement of the large intra-abdominal vessels with grafts in order to achieve the R0 resection. In these techniques sometimes there is absence of specific training. To achieve best results for RSTS patients, the presence of an experienced vascular surgeon during such operations is of paramount importance to aid in prolonging the overall survival of patients.
REFERENCES
- Gronchi A, Strauss C, Miceli R, Bonvalot S, Swallow C.J, Hohenberger, P et al. Variability in Patterns of Recurrence After Resection of Primary Retroperitoneal Sarcoma (RPS): A Report on 1007 Patients From the Multi-institutional Collaborative RPSWorking Group. Ann. Surg 2016;263:1002-9.
- Gamboa AC, Gronchi A, Cardona Soft-tissue sarcoma in adults: An update on the current state of histiotype-specific management in an era of personalized medicine. CA Cancer J Clin 2020;70:200-29.
- Sbaraglia M, Bellan E, Dei Tos AP. The 2020 WHO Classification of Soft Tissue Tumours: news and perspectives. Pathologica 2021;113:70-84.
- Carbone, F, Pizzolorusso A, Di Lorenzo G, Di Marzo, M, Cannella, L, Barretta, ML, et Multidisciplinary Management of Retroperitoneal Sarcoma: Diagnosis, Prognostic Factors and Treatment. Cancers 2021;13:4016.
- Improta L, Tzanis D, Bouhadiba T, Abdelhafidh K, Bonvalot Overview of primary adult retroperitoneal tumours. Eur J Surg Oncol 2020;46:1573-9.
- Dai N, Yuan J, Wang X, Bai H, Ding H, Li X et al. Giant Intra-Abdominal Tumor, Compatible with Liposarcoma: A Case Report and Literature Review. Am J Case Rep 2025;26:948952.
- Homsy P, Blomqvist C, Heiskanen I, Vikatmaa L, Tukiainen E, Numminen K et al. Multidisciplinary Oncovascular Surgery is Safe and Effective in the Treatment of Intra-abdominal and Retroperitoneal Sarcomas: A Retrospective Single Centre Cohort Study and a Comprehensive Literature Review. Eur J Vasc Endovasc Surg 2020;60:752-763.
- Bree, E, Michelakis D, Heretis I, Kontopodis N, Spanakis K, Lagoudaki, E et al. Retroperitoneal Soft Tissue Sarcoma: Emerging Therapeutic Strategies. Cancers 2023;15:5469.
- Balaz P, Whitley A, Heinola I, Gargiulo M, Vikatmaa OVS Collaborative Author Group. Surgical Management of Tumours Invading the Inferior Vena Cava: A Delphi Consensus Document. Eur J Vasc Endovasc Surg 2025;70:389-99.
- Yoo HJ, Hong SH, Kang Y, Choi JY, Moon KC, Kim HS et al. MR imaging of myxofibrosarcoma and undifferentiated sarcoma with emphasis on tail sign; diagnostic and prognostic value. Eur Radiol 2014;24:1749-57.
- Yokoyama Y, Nishida Y, Ikuta K, Nagino M. A case of retroperitoneal dedifferentiated liposarcoma successfully treated by neoadjuvant chemotherapy and subsequent surgery. Surg Case Rep 2020;246:105.
- Von Mehren M, Kane JM, Agulnik M, Bui MM, Carr-Ascher J, Choy E et Soft Tissue Sarcoma, Version 2.2022, NCCN Clinical Practice Guidelines in Oncology J Natl Compr Canc Netw 2022;20:815-833.
- Judson I, Verweij J, Gelderblom H, Hartmann JT, Schöffski P, Blay JY et al. European Organisation and Treatment of Cancer Soft Tissue and Bone Sarcoma Doxorubicin alone versus intensified doxorubicin plus ifosfamide for first-line treatment of advanced or metastatic soft-tissue sarcoma: a randomised controlled phase 3 trial. Lancet Oncol 2014;15:415-23.
- Fabbroni C, Grignani G, Vincenzi B, Fumagalli E, De Pas TM, Mazzocca A et al. TRAbectedin in adVanced rEtroperitoneal well differentiated/dedifferentiated Liposarcoma and Leiomyosarcoma (TRAVELL): results of a phase II study from the Italian Sarcoma Group. ESMO Open 2024;9:103667.
- Martin-Broto J, Martinez-Garcia J, Moura DS, Redondo A, Gutierrez A, Lopez-Pousa A et al. Phase II trial of CDK4/6 inhibitor palbociclib in advanced sarcoma based on mRNA expression of CDK4/ Signal Transduct Target Ther 2023;8:405.
- Gounder MM, Bauer TM, Schwartz GK, Weise AM, LoRusso P, Kumar P et al. A First-in-Human Phase I Study of Milademetan, an MDM2 Inhibitor, in Patients With Advanced Liposarcoma, Solid Tumors, or J Clin Oncol 2023;41:1714-24.
- Tseng, W, Barretta, F, Conti, L, Grignani, G, Tolomeo F, Albertsmeier M et al. Defining the role of neoadjuvant systemic therapy in high-risk retroperitoneal sarcoma: A multi-institutional study from the Transatlantic Australasian Retroperitoneal Sarcoma Working Group. Cancer 2021;127:729-38.
- Bonvalot S, Gronchi A, Le Péchoux C, Swallow CJ, Strauss D, Meeus P et Preoperative radiotherapy plus surgery versus surgery alone for patients with primary retroperitoneal sarcoma (EORTC-62092: STRASS): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol 2020;21:1366-77.
- Stoeckle E, Coindre JM, Bonvalot S, Kantor G, Terrier P, Bonichon F et al. French Federation of Cancer Centers Sarcoma Prognostic factors in retroperitoneal sarcoma: a multivariate analysis of a series of 165 patients of the French Cancer Center Federation Sarcoma Group. Cancer 2001;92:359-68.
- Swallow, J., Strauss, D.C., Bonvalot, S., Rutkowski, P., Desai, A., Gladdy et al.. Management of primary retroperitoneal sarcoma (RPS) in the adult: an updated consensus approach from the Transatlantic Australasian RPS Working Group. Annals of surgical oncology 2021;28:7873.
- Devaud NA, Butte JM, De la Maza JC, von Mühlenbrock Hugo S, Cardona Complex Vascular Resections for Retroperitoneal Soft Tissue Sarcoma. Curr Oncol 2023;30:3500-15.
- Hasegawa S, Nomura Y, Okada T, Toyama H, Fukumoto T, Okada K. Complete resection and arterial reconstruction for primary sarcoma arising from superior mesenteric J Vasc Surg Cases Innov Tech 2021;8:70-74.
- Carbone, F.; Pizzolorusso, A.; Di Lorenzo, G.; Di Marzo, ; Cannella, L.; Barretta, M.L.; Delrio, P.; Tafuto, S. Multidisciplinary Management of Retroperitoneal Sarcoma: Diagnosis, Prognostic Factors and Treatment. Cancers 2021;13:4016.
- Kotsis T, Papadopoulos A, Memos N. Stepwise Surgical Strategy for Retroperitoneal Myxofibrosarcoma with Inferior Vena Cava Reconstruction Prior to En Bloc Resection: A Case Report. Vasc Specialist Int 2025;41:7.
- Zahiri A, Fereydooni A, Eshraghian E, Ho M, Delitto D, Lee B, Poultsides GA. The Two-Decade Experience of Oncovascular Reconstruction in Patients with Retroperitoneal Sarcoma. Ann Vasc Surg 2025;121:543-54.
- Ferraris, M, Callegaro, D, Barretta, F, Fiore, M, Radaelli, S, Stacchiotti, S ET AL. Outcome of iliocaval resection and reconstruction for retroperitoneal sarcoma. J Vasc Surg Venous Lymphat Disord 2019;7:547-56.
- Grieff AN, Hamilton C, Ady J, Beckerman WE, Shafritz R, Koshenkov V et Concomitant Aorto-Caval Reconstruction for Inferior Vena Cava Leiomyosarcoma. Ann Vasc Surg 2021;70:567.e13-567.e17.
- Li WX, Tong HX, Lv CT, Yang H, Zhao G, Lu WQ et Management of retroperitoneal sarcoma involving the iliac artery: Single-center surgical experience. World J Clin Cases 2022;10:811-19.
- Quildrian SD, Nardi WS, David M. Resection of retroperitoneal soft-tissue sarcoma involving the abdominal BMJ Case Rep 2020;13:237107.
- Bael P, Alqtishat B, Alshawwa K. Case Report: Successful R0 resection in locally advanced retroperitoneal sarcomas. Front Surg. 2024;11:1343014.
- Castro IF, Nunes PHS, Lopes ACX, Lima MC, Conrado RP, Leal RMLV et Surgical resection of retrohepatic inferior vena cava leiomyosarcoma without vascular reconstruction: case report. J Vasc Bras 2023;22:e20220108.
- Tirnavean O, Van Bellinghen C, Monfort L, Coulier B, Buche M, Papadatos S, e al. Inferior vena cava reconstruction with a superficial femoral vein graft after resection of a venous leiomyosarcoma. Acta Chir Belg 2021;121:144
- Schwarzbach, M.H, Hormann, Y, Hinz, U, Leowardi, C, Bockler, D, Mechtersheimer, G et Clinical results of surgery for retroperitoneal sarcoma with major blood vessel involvement. J Vasc Surg 2006;44:46-55.
- Li CP, Liu BN, Wu JH, Hao CY. Contralateral internal iliac artery transposition for retroperitoneal sarcoma involving common iliac artery. Updates Surg 2022;74:1157-63.
- Kontopodis N, Bree E, Michelakis D, Ioannou CV. Oncovascular Resection and Reconstruction of Recurrent Retroperitoneal Liposarcoma Adherent to the Iliac Veins and Vena Cava. Vasc Specialist Int 2021;37:58-9.
- Kakkos S, Kirkilesis G, Caprini JA, Geroulakos G, Nicolaides A, Stansby G et al. Combined intermittent pneumatic leg compression and pharmacological prophylaxis for prevention of venous thromboembolism. Cochrane Database Syst Rev 2022 Jan 28;1(1):CD005258.
{kind=link}