When even luck matters: a compendium of all possible complications during hybrid repair of a dissecting TAAA occurred in a single patient

| Available Online: | September, 2023 |
| Page: | 65-67 |
Author for correspondence:
Federico Pascucci, MD
Viale Cappuccini, 1 – 71013- San Giovanni Rotondo (FG), Italy
Email: fedepascucci@libero.it
doi: 10.59037/hjves.v5i2.49
ISSN: 2732-7175 / 2023 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications
All rights reserved. https://www.heljves.com
Federico Pascucci 1,2, Giovanni Mastrangelo 1, Vincenzo Palazzo 1
1 Department of Vascular Surgery, Casa Sollievo della Sofferenza, San Giovanni Rotondo
2 School of Vascular Surgery, Università Cattolica del Sacro Cuore, Roma
Abstract
Full Text
References
Images
Abstract
Abstract:
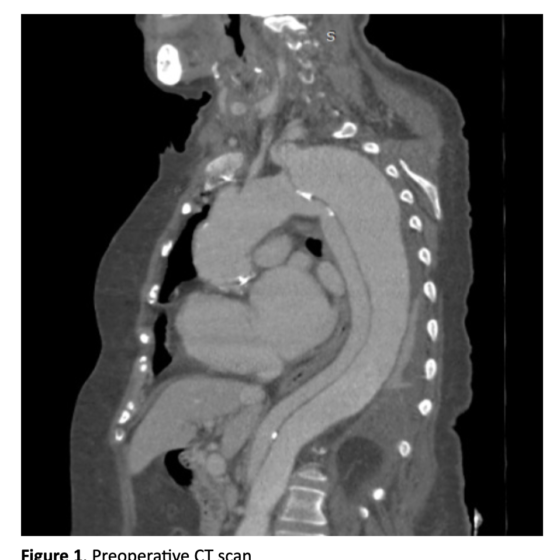
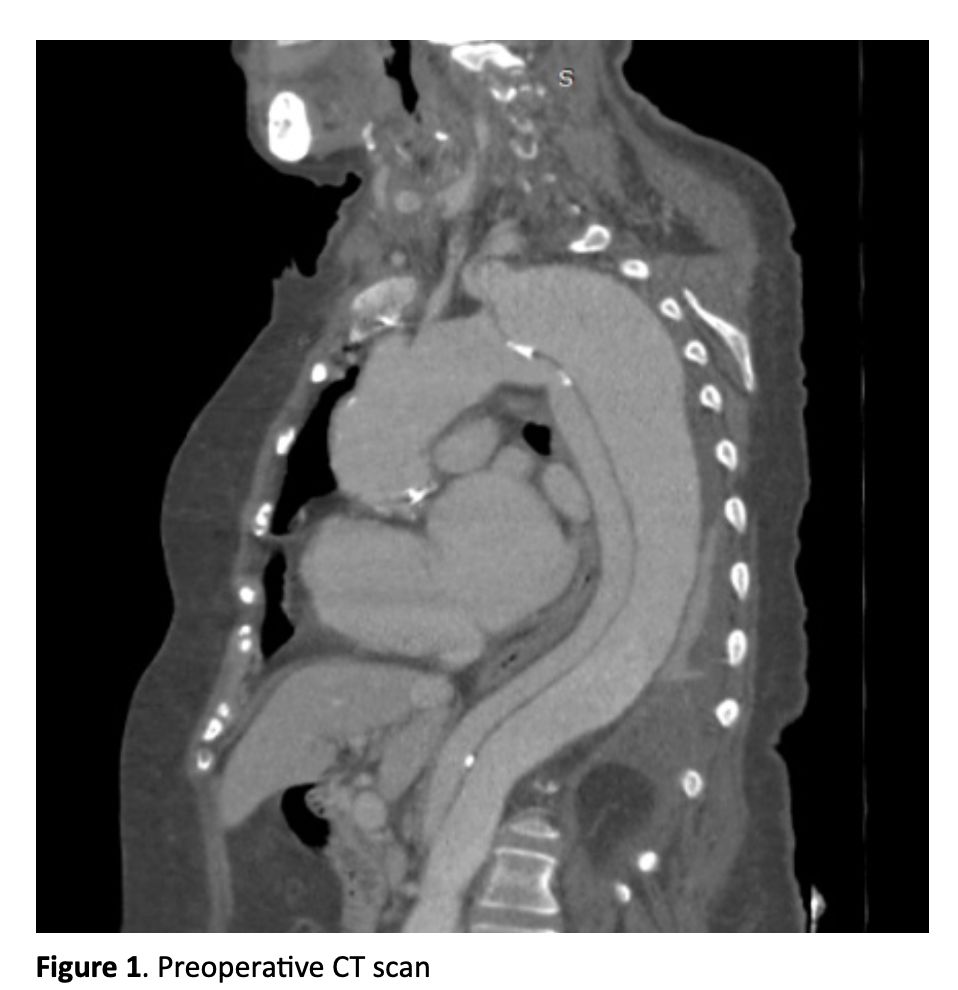
Purpose: A 73-year-old woman, already submitted to repair of the ascending aorta and subsequently to aortic valve substitution in redo sternotomy, presented to our attention with a dissecting TAAA with a distal aortic arch diameter of 6 cm. Our goal was to offer this extremely fragile patient the least invasive surgical treatment as possible.
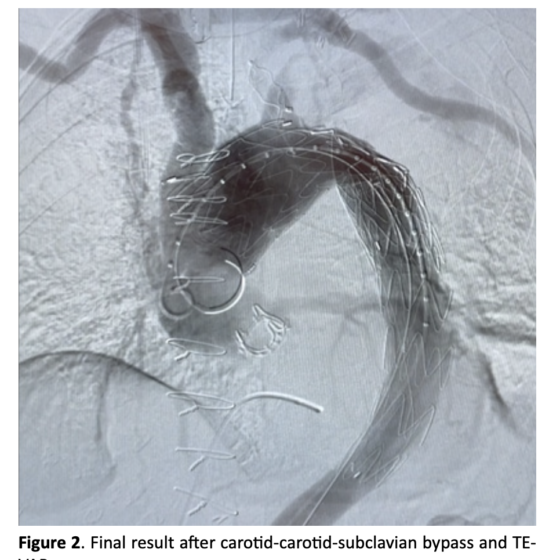
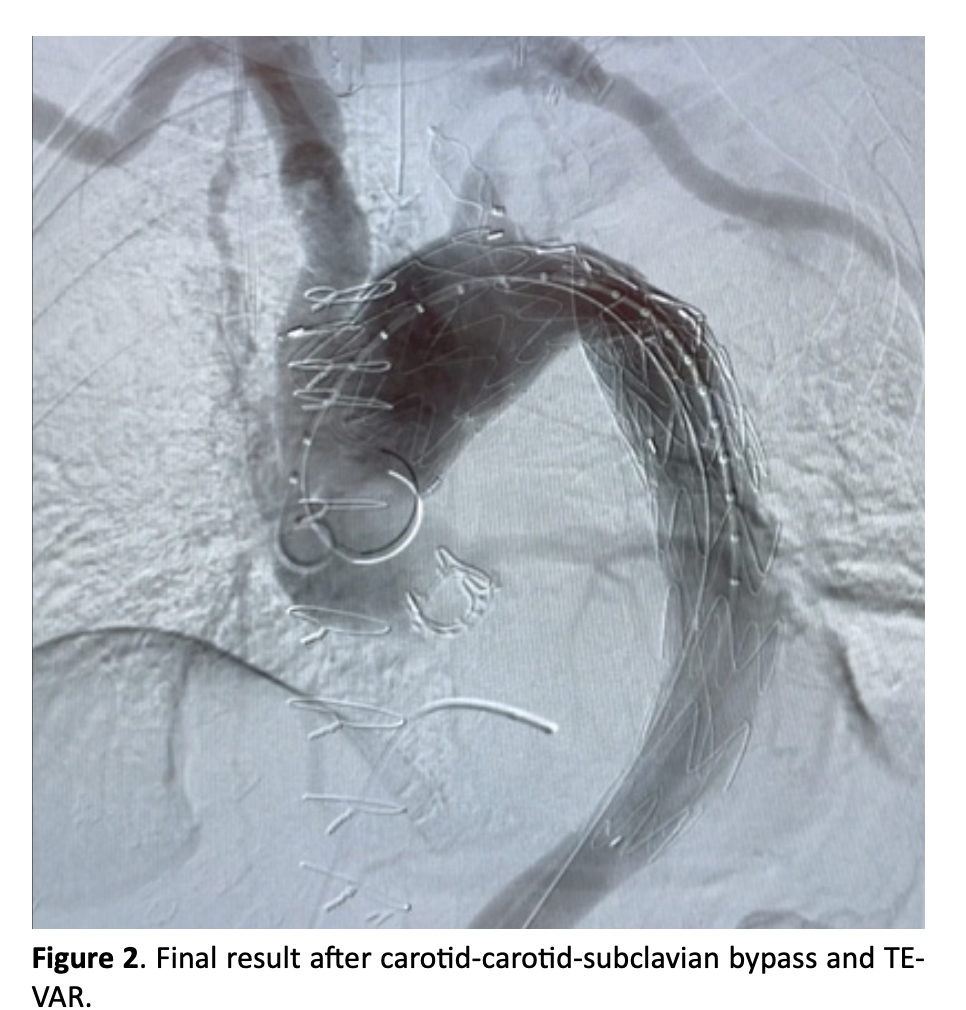
Technique: We treated this patient in two stages. In the first stage we performed a carotid-carotid-subclavian bypass. In the second stage we performed a TEVAR in zone 1, extending from the brachiocephalic artery to the celiac trunk. Left subclavian artery was previously occluded with a plug. CSFD was not adopted by default.
Conclusion This patient reported some extremely rare and unexpected complications that brought us to report this case. Hybrid techniques represent an extremely appealing opportunity to treat fragile patients affected by complex aortic diseases with relatively little invasive strategies, however, serious complications can occur even after these surgeries.
Full Text
INTRODUCTION
Repair of dissecting thoracoabdominal aortic aneurysms (TAAAs) involving the distal aortic arch remains challenging, especially in fragile patients. When traditional open repair cannot be performed, hybrid surgery represents an excellent therapeutic option. 1 Supra aortic trunks debranching associated with TEVAR has become in the last years one of the most used techniques for the treatment of aortic arch diseases, with excellent patency rates of extra anatomic bypasses and good clinical midterm result. However, these procedures are technically demanding and bring relevant rates of complications. 2 In adjunct, proximal endograft deployment brings a not negligible risk of type IA endoleak. 3
We present the case of a 73-year-old woman, already submitted in emergency setting to repair of the ascending aorta for a type A aortic dissection and subsequently to aortic valve substiution for valvular degeneration in a redo sternotomy. In anamnesis she also reported: atrial fibrillation, hypertension, left nephrectomy for bleeding hemangioma and abdominoperineal resection for anorectal malignant melanoma. The patient presented to our attention with a residual dissecting TAAA with a distal aortic arch diameter of 6 cm. Our goal was to offer to this extremely fragile patient the least invasive surgical treatment as possible.
TECHNIQUE
To split the surgical stress burden, we decided to treat this fragile patient in two different stages. In the first stage we performed a carotid-carotid-subclavian bypass using a 8 mm non-ringed ePTFE graft (Propaten, WL Gore, Flagstaff, AZ, USA). The graft was tunneled in the subcutaneous tissue without torsion or kinking. The patient was discharged home and subsequently readmitted after one month. In the second stage we performed a TEVAR in zone 1 with two overlapping tapered thoracic endografts (Bolton Relay Plus, Terumo Aortic, Vascutek Ltd., Inchinnan, UK), extended from the origin of the brachiocephalic artery to the origin of the celiac trunk. Left subclavian artery was previously occluded with a plug (Amplatzer Vascular Plug, St. Jude Medical Inc., St. Paul, MN, USA) at the beginning of the same procedure. CSFD was not adopted by default before initiating the procedure. Residual dissection of the abdominal aorta, with all the visceral vessels originating from the true lumen and a small aortic diameter, was not considered to be in need of treatment.
DSCUSSION
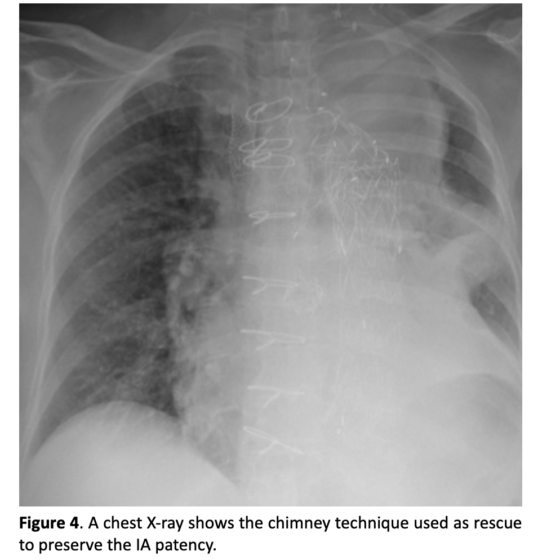
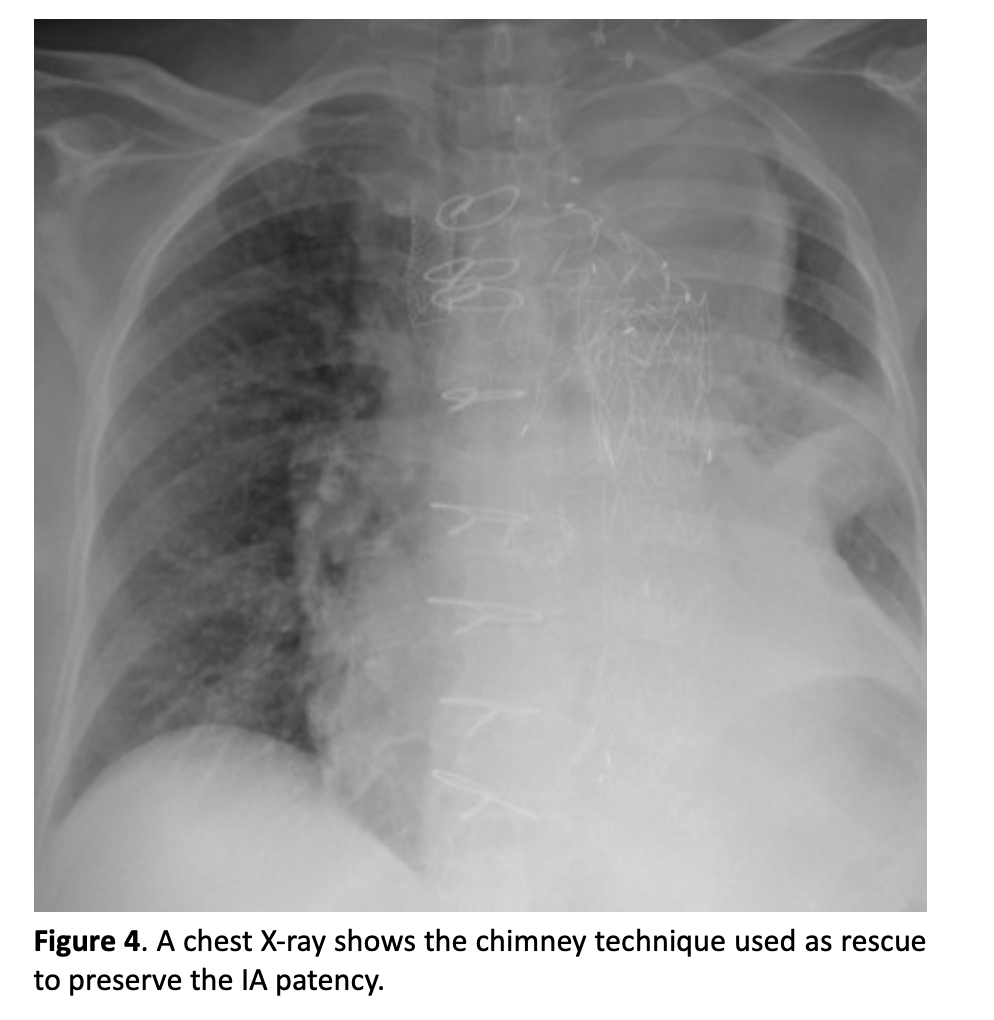
During the two postoperative courses this patient reported some extremely rare and unexpected complications that brought us to report this case. After the first intervention, on postoperative day (POD) 2, she developed a complete deficit in the pronation-supination and flexion-extension of the left arm: the electroneurography showed a transient stupor of brachial plexus, completely resolved after a few weeks with medical therapy and motor rehabilitation. On POD 6 the patient started developing progressive anemia, initially treated with red blood cell transfusions. On POD 8 she was submitted to an urgent CT scan, that revealed an enormous pelvic hematoma originating from a spontaneous rupture of the external iliac artery, treated with a covered stent (Viabahn, WL Gore, Flagstaff, AZ, USA) with excellent result. In adjunct, during postoperative course, the patient contracted Sars-CoV-2 infection, requiring NIV for a few days. The second stage (TEVAR) was completed with a good angiographic result and without complications of any type. Patient was close to be discharged home when, on POD 3, she suddenly developed bilateral brachial hypotension, malaise and mental confusion. An urgent CT scan was performed and an almost complete coverage of the brachiocephalic artery by the most proximal endograft was observed. The patient was urgently submitted to an endovascular relining of the brachiocephalic artery using two imbricated balloon expandable covered stents (VBX, WL Gore, Flagstaff, AZ, USA) post dilated with a semi-compliant valvuloplasty balloon, with good angiographic results and complete remission of symptoms.
CONCLUSION
Hybrid techniques offer vascular surgeons an extremely appealing opportunity to treat fragile patients affected by com- plex thoracoabdominal aortic diseases with relatively little invasive strategies. Despite this, as we experienced with this patient, serious complications can occur even after these surgeries. Prompt recognition and treatment of these complications should be in the armamentarium of the hybrid vascular surgeon. In particular, early proximal endograft migration is a complication not yet described in literature that can occur, as we experienced. Forces acting on proximally deployed endograft are complex and could have various effect, more often a distal migration of the endograft.4 However, it seems necessary to us a better comprehension of possible interactions be- tween endograft and native aortic arch.5 More advanced total endovascular strategies are spreading quickly but long-term data are still lacking on this specific argument. 6
References
- Martin G, Riga C, Gibbs R, Jenkins M, Hamady M, Bicknell C. Short- and Long-term Results of Hybrid Arch and Proximal Descending Thoracic Aortic Repair: A Benchmark for New Technologies. J Endovasc Ther. 2016;23(5):783-790. doi:10.1177/1526602816655446
- Parker MH, Colpitts DK, Gilson GF, Ryan L, Mukherjee D. Carotid-Axillary Bypass as an Alternative to Carotid-Subclavian Bypass Following Coverage of Left Subclavian Artery During TEVAR. https://doi. org/101177/1538574420983655. 2020;55(3):265-268. doi:10.1177/1538574420983655
- Scurto L, Peluso N, Pascucci F, et al. Type 1A Endoleak after TEVAR in the Aortic Arch: A Review of the Literature. J Pers Med. 2022;12(8). doi:10.3390/JPM12081279
- Skrypnik D, Kalmykov E, Bischoff MS, et al. Late Endograft Migration After Thoracic Endovascular Aortic Repair: A Systematic Review and Meta-analysis. J Endovasc Ther. Published online 2022. doi:10.1177/15266028221109455
- Domanin M, Bissacco D, Romarowsky RM, et al. Drag Forces after Thoracic Endovascular Aortic Repair. General Review of the Literature. Ann Vasc Surg. 2021;75:479- 488. doi:10.1016/J.AVSG.2021.02.042
- Canaud L, Chassin-Trubert L, Abouliatim I, et al. Total Arch Thoracic Endovascular Aortic Repair Using Double Fenestrated Physician-Modified Stent-Grafts: 100 Patients. J Endovasc Ther. Published online 2022. doi:10.1177/15266028221116747

{kind=link}
{kind=link}
{kind=link}
{kind=link}