Ruptured aneurysm of left colic artery: A case report

| Available Online: | May, 2023 |
| Page: | 20-22 |
Author for correspondence:
Apostolos Chaveles
Department of Vascular Surgery, KAT General Hospital, 2 Nikis Street, Kifisia, 14561, Athens, Greece
E-mail: chaveles.apostolos@gmail.com
doi: 10.59037/hjves.v5i1.29
ISSN 2732-7175 / 2023 Hellenic Society of Vascular and Endovascular Surgery Published by Rotonda Publications
All rights reserved. https://www.heljves.com
Chaveles A.1 , Anastasiadou Ch.1 , Maltezos K.1 , Pachi A.1 , Tzortzis D.2 , Doukogianni I.1 , Papapetrou A.1 , Kerasidis S.1 , Papacharalampous G.1 , Maltezos Ch.1
1 Department of Vascular Surgery, KAT General Hospital, Athens, Greece
2 Department of Interventional Radiology, KAT General Hospital, Athens, Greece
Abstract
Full Text
References
Images
Abstract
Abstract:
Visceral artery aneurysms belong among the rarest aneurysms, while only few cases of left colic artery aneurysms have been described. We present a case of a ruptured aneurysm of left colic artery in a 52 year old woman. The patient was managed successfully by endovascular means. The post operative course was uneventful and the patient was discharged from the hospital on the 7th postoperative day.
Full Text
CASE REPORT
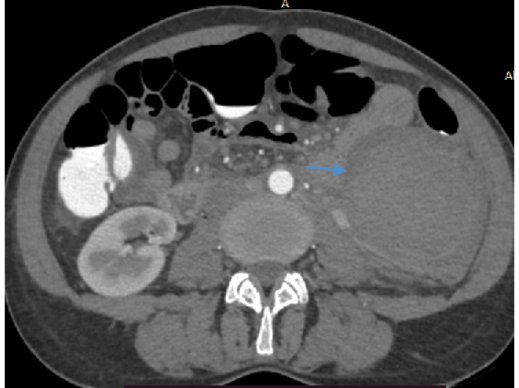
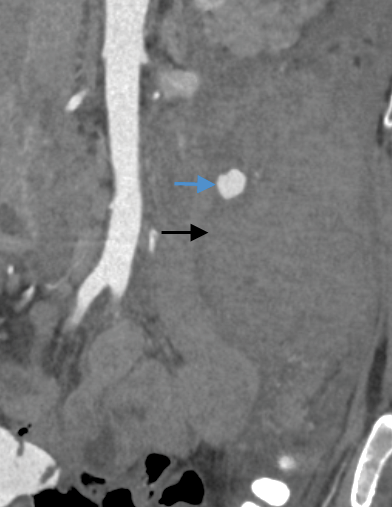
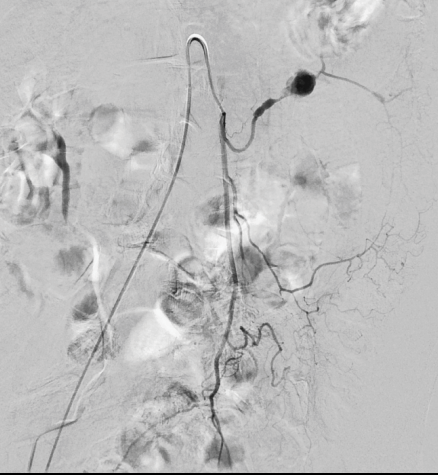
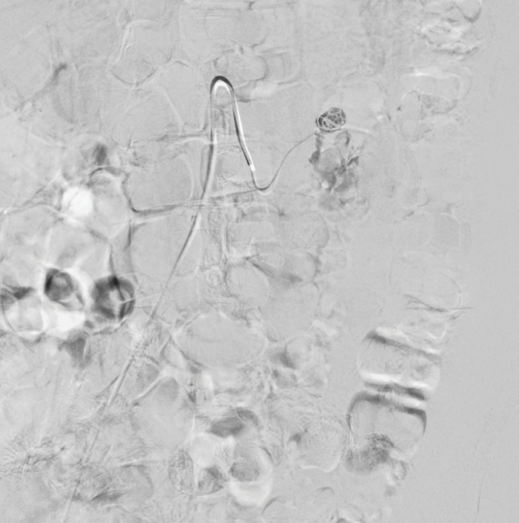
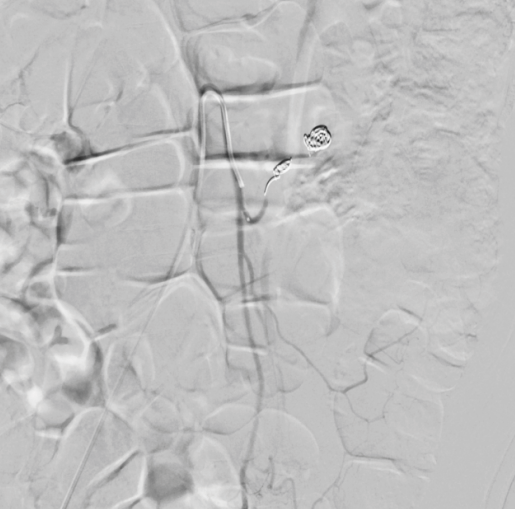
*A 52 year old female patient with medical history of hypothyroidism and tobacco abuse (60 pack years ) presented to the emergency department of another hospital complaining about hypogastric – left lower quadrant abdominal pain. Blood tests, arterial blood gas analysis, abdominal and transvaginal ultrasound were normal. The patient was admitted and treated with intravenous antibiotics (ceftriaxone, ciprofloxacin, metronidazole) like an intra-abdominal inflammation, and symptoms were relieved after 48 hours. On the 3rd day of hospitalization, the patient had acute hypogastric – left lumbar abdominal pain and an episode of orthostatic hypotension. At the same time, a complete blood count showed a drop in hemoglobin / hematocrit (Hgb 9.5 g/dL ,Hct 28.4%) with no hemodynamic changes in the status of the patient. Clinical examination revealed pain elicited by palpation of the left lumbar region with a palpable mass and positive Blumberg sign. A Computed Tomography Angiography (CTA) was performed revealing a ruptured left colic artery aneurysm (maximum diameter = 1.1 cm) with a retroperitoneal hematoma (8.3 cm x 7 cm) (Fig. 1 and 2). The patient was hemodynamically stable and was transferred to our hospital where she underwent angiography. Percutaneous access from the right common femoral artery was gained under local anesthesia and selective cannulation of the inferior mesenteric artery first and then of the left colic artery was achieved with a vertebral catheter. Diagnostic angiography confirmed the presence of an aneurysm of the left colic artery (Fig. 3). Embolization of the aneurysm sac was achieved with multiple microcoils (Hilal Embolization Microcoils 18S- 4.0 cm – 6 mm – COOK MEDICAL ) (Fig. 4). Additionally, embolization of the left colic artery proximal to the aneurysm sac was performed with the same pushable microcoils (Fig. 5). Postoperatively the patient was transferred to the ward for further treatment. Over the following day, complete blood count showed elevation of white blood cells (WBC 18,300, Neu 82%) and further drop in hemoglobin / hematocrit (HgB 8.7 g/dL, Hct 27%), whereas physical examination of the patient revealed persistent hypogastric abdominal pain. Arterial Blood Gas test showed no abnormalities (normal range of pH and lactate). Contrast-enhanced abdominal computed tomography scan was performed and showed a slight increase in the dimensions of the retroperitoneal hematoma (9.5 cm x 7 cm) with no active extravasation. No signs of colonic ischemia were found. The patient was treated conservatively with intravenous antibiotics (piperacillin/tazobactam, metronidazole) and fluids , with gradual relief of symptoms. She was discharged from our department on the 7th postoperative day. Abdominal computed tomography after 6 months showed decrease of the dimensions of the retroperitoneal hematoma (3.8 cm x 4 cm) while the patient remained free of symptoms.
DISCUSSION
Visceral aneurysms belong among the rarest aneurysms with an incidence of 0.2-2% in the general population.1-4 Splenic and hepatic aneurysms are the most common visceral aneurysms while inferior mesenteric artery aneurysms and its branches are extremely rare and account for less than 1% of all splanchnic aneurysms.5 Only a few cases of left colic artery aneurysm have been described in the literature. The pathogenesis of these aneurysms is not well understood, although various causes of splanchnic aneurysms have been proposed, including atherosclerosis, medial degeneration, collagen diseases (Ehlers-Danlos syndrome), vasculitis (Takayasu, Polyarteritis nodosa) fibromuscular dysplasia and autoimmune disorders.6,7 A male predominance of 5:1 has been reported.8 Most of the cases remain asymptomatic and the aneurysm is randomly discovered during an investigation for another abdominal pathology. Some cases, however, have presented in the emergency department with rupture as a medical emergency, with abdominal pain and hypovolemic shock. In these cases, mortality seems to be 20%9 although it has been reported that in urgent surgery mortality can be increased up to 70%.10 Diagnosis is often made with computed tomography angiography (CTA) while other imaging techniques such as Magnetic Resonance Angiography (MRA), Digital Subtraction Angiography (DSA) or even ultrasound could be used.11 Latest guidelines report that mesenteric branch artery aneurysms should be treated regardless of size.12-14 In the past, open surgery with resection of the aneurysm with or without bypass procedure was the treatment of choice for these entities. Nowadays, endovascular techniques have been described for the treatment of visceral aneurysms, including the use of stent grafts, coil and N-butyl-2-cyanoacrylate (n-BCA) acrylic glue. Given the fact that only few cases of aneurysms of the mesenteric artery branches have been reported, there are no large studies comparing the results and the most appropriate treatment. However, various case reports have showed great results with endovascular treatment, instead of the classic open surgery, minimizing mortality, morbidity and the duration of hospitalization of the patients and should be the considered as the treatment of choice.
CONCLUSION
Inferior mesenteric artery aneurysms and mesenteric branches artery aneurysms are rare entities. Any encountered lesion should be treated regardless of size. There are no large studies indicating the treatment of choice although latest results have showed that endovascular treatment should be considered as the first line of treatment for these patients even if rupture has occurred.
References
- Hossain A, Reis ED, Dave SP, Kerstein MD, Hollier LH. Visceral artery aneurysms: experience in a tertiary-care center. Am Surg 2001;67:432-7.
- Upchurch GR Jr, Zelenock GB, Stanley JC. Splanchnic artery aneurysms. In Rutherford RB, ed. Vascular Surgery, 6th ed. Philadelphia, PA: Saunders; 2005; pp 1565-81.
- Saltzberg SS, Maldonado TS, Lamparello PJ, Cayne NS, Nalbandian MM, Rosen RJ, et al. Is endovascular therapy the preferred treatment for all visceral artery aneurysms? Ann Vasc Surg 2005;19:507-15.
- Berceli SA. Hepatic and splenic artery aneurysms. Semin Vasc Surg 2005;18:196-201.
- Messina LM, Stanley CJ. Visceral artery aneurysm. In: Gewerz BL, Schwartz LB, eds. Surgery of the aorta and its branches. Philadelphia,PA: Saunders; 2000; pp 358-65.
- Girishkumar H. et al: Aneurysm of the right colic artery. J Cardiovasc Surg 1997;38:305-7.
- Busuttil RW, Brin BJ. The diagnosis and management of visceral artery aneurysms. Surgery 1980;88:619-24.
- Davidovic LB, Vasic DM, Colic MI. Inferior mesenteric artery aneurysm: case report and review of the literature. Asian J Surg 2003;26:176-9.
- Shanley CJ, Shah NL, Messina LM. Uncommon splanchnic artery aneurysms: pancreaticoduodenal, gastroduodenal, supe rior mesenteric, inferior mesenteric, and colic. Ann Vasc Surg 1996;10:506-15.
- Khan S, Cheatle T. Left gastric artery aneurysm–a case report. Eur J Vasc Endovasc Surg 1997;14:413-4.
- Yoo BR, Han HY, Cho YK, Park SJ. Spontaneous rupture of a middle colic artery aneurysm arising from superior mesenteric artery dissection: Diagnosis by color Doppler ultrasonography and CT angiography. J Clin Ultrasound 2012;40:255-9.
- Goffi L, Chan R, Boccoli G, Ghiselli R, Saba V. Aneurysm of a jejunal branch of the superior mesenteric artery in a patient with Marfan’s syndrome. J Cardiovasc Surg (Torino) 2000;41:321-3.
- Messina LM, Shanley CJ. Visceral artery aneurysms. Surg Clin North Am 1997;77:425-42.
- Tessier DJ, Abbas MA, Fowl RJ, Stone WM, Bower TC, McKusick MA, Gloviczki P. Management of rare mesenteric arterial branch aneurysms. Ann Vasc Surg 2002;16:586-90.